Actinic keratosis
Authors:
Mikael Häggström; Authors of integrated Creative Commons article[1] [note 1]
Actinic keratosis may present as suspected malignant skin excisions.
Contents
Fixation
Generally 10% neutral buffered formalin.
See also: General notes on fixation
Gross processing

Gross examination
Note:
- Color
- Well-defined or diffuse border
- Size
- Any elevation
Lesions of actinic keratosis are typically ill-marginated, erythematous, scaling, and rough papules or patches. These will typically be found in areas displaying other signs of solar damage, such as atrophy, uneven pigmentation, and telangiectasias.[1]
Tissue selection
| <4 mm | 4 - 8 mm | 9 - 15 mm |
|---|---|---|

|

|

|
In table above, each top image shows recommended lines for cutting out slices to be submitted for further processing. Bottom image shows which side of the slice that should be put to microtomy. Dashed lines here mean that either side could be used. Further information: Gross processing of skin excisions
Microscopic evaluation
- Evaluation mainly consists of:
- Establishing a diagnosis of actinic keratosis rather than differential diagnoses:
- Excluding any presence of cutaneous squamous cell carcinoma in the lesion.
Characteristics


By definition, actinic keratosis is confined to foci within the epidermis.[1]
it also generally has:[1]
- Aggregates of atypical, pleomorphic keratinocytes which show nuclear atypia, dyskeratosis, and loss of polarity.
- Hyperkeratosis and parakeratosis, the latter overlying the abnormal cells in the epidermis. Due to the sparing of segments of the epithelium overlying adnexal structures, a characteristic pattern of alternating orthokeratosis and parakeratosis, referred to as the “flag-sign,” can often be seen (Figure 1(a)).
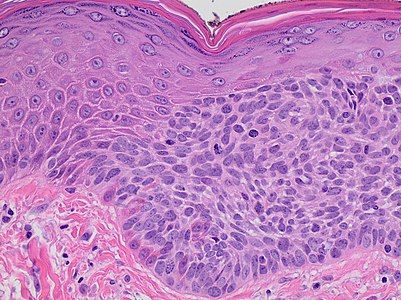
- Atypical keratinocytes will not span the full thickness of the epidermis (Figure 1(b)), although those in the basal cell layer will frequently extend into the granular and cornified layers. The exception to this criterion is the Bowenoid variant of actinic keratosis, which resembles cutaneous squamous-cell carcinoma in situ (Bowen's disease) but is less disordered with less nuclear atypia and crowding.
- A more basophilic basal layer than normal, which is generally thought to be a consequence of the close crowding of atypical keratinocytes (Figure 1(b)).
- Some cases will also show basal layer degeneration and the formation of Civatte bodies (Figure 1(c)), the result of a lichenoid infiltrate with irregular acanthosis. This can be distinguished from lichenoid dermatitis by the presence of keratinocyte atypia.
- Dermoepidermal junction irregularities, with small round buds at the basal cell layer that will protrude slightly into the upper papillary dermis (Figure 1(d)).
- There is almost always an associated solar elastosis in the dermis, and a lack thereof can often be sufficient to prompt reconsideration of the diagnosis.

1(b). Early actinic keratosis with keratinocyte dysplasia confined to the lower third of the epidermis.[1]

Civatte body (in a case in lichen planus).

1(d). A more established lesion of actinic keratosis demonstrating nearly full thickness keratinocyte dysplasia and prominent budding of the basal layer into the superficial dermis.[1]



Squamous cell-like skin proliferations: Differential diagnosis
Main differential diagnoses and their characteristics:[3]

Invasive squamous-cell carcinoma of the skin: Atypical and pleomorphic keratinocytes, involving the dermis and the sub-cutis with a potential metastatic spread.

Squamous-cell carcinoma in situ (Bowen’s disease): Atypical keratinocytes at every layer of epidermis.
Actinic keratosis: Atypical keratinocytes that do not span the full thickness of the epidermis (or, in Bowenoid variant, are less disordered with less nuclear atypia and crowding).

Keratoacanthoma: Symmetrical and circumscribed proliferation of keratinocytes, with central horn plug, with epidermis that extends over the tumor. It can be regarded as a highly differentiated SCC.

Crush artifacts: Needles used to orient the skin sample may create crush artifacts (black arrow) mimicking cellular atypia with mainly hypereosinophilia and nuclear pleomorphism. Image also shows folding artifacts (white arrows).

Adnexal carcinomas: Squamous differentiation, but does not show connection with the epidermis and highlights adnexal features.

Adenosquamous carcinoma: Mixed glandular and squamous differentiation.

Verruca vulgaris: Marked hyperkeratosis and papillomatosis. Rete ridges slope inward at the borders of the lesion.

Verrucous squamous cell carcinoma[note 3]: Exophytic squamous proliferation with marked papillomatosis and low atypia and the presence of koilocyte-like changes. Found in head and neck locations, as well as in the genitalia and sole of the foot.

Inverted follicular keratosis:[note 4]: Sharply circumscribed endophytic verrucous proliferation with prominent squamous features.

Seborrheic keratosis: Acanthosis, absence of atypia, pseudo-horn cysts, in inflamed lesions, mitoses may be present.

Bowenoid papulosis: Atypical keratinocytes and mitoses. Histology similar to Bowen’s disease.

A melanoma may have relatively plentiful eosinophilic cytoplasm, and be seemingly continuous with the squamous epithelium (at left in image), thus resembling a squamous cell carcinoma. However, the nesting of cells at right in the image is more characteristic of a melanoma.

Metastasis: Personal medical history of the patient, nodular proliferation without connection to epidermis, immunohistochemical evaluation. Squamous-cell carcinoma metastasis from lungs to the skin is pictured.


.jpg)



.jpg)






Clinical clues
- Biopsy from sun exposed area (including the face, neck, dorsal hands, and forearms, upper chest, back, and scalp).[1]
- Generally middle-aged or older individuals.[1]
Further workup
Once a diagnosis of actinic keratosis is established, optionally characterize the degree of atypia into either mild, moderate or severe.
Histopathology report
- Objective findings
- A diagnosis of actinic keratosis
- Optionally: The degree of atypia.
- Even absence of evidence of malignancy.
Example for the case in "Further workup":
 |
See also: General notes on reporting
Notes
- ↑ For a full list of contributors, see article history. Creators of images are attributed at the image description pages, seen by clicking on the images. See Patholines:Authorship for details.
- ↑ The excision example shows a superficial basal cell carcinoma.
- ↑ - Buschke–Löwenstein tumor is an alternative name for verrucous squamous cell carcinoma in the ano-genital region.
- Carcinoma cuniculatum is a characteristic form of verrucous squamous cell carcinoma on the sole. - ↑ Inverted follicular keratosis is generally thought to be a rare variant of seborrheic keratosis, but this position is not universally accepted.
- Karadag, AyseSerap; Ozlu, Emin; Uzuncakmak, TugbaKevser; Akdeniz, Necmettin; Cobanoglu, Bengu; Oman, Berkant (2016). "Inverted follicular keratosis successfully treated with imiquimod ". Indian Dermatology Online Journal 7 (3): 177. doi:. ISSN 2229-5178.
Main page
References
- ↑ 1.0 1.1 1.2 1.3 1.4 1.5 1.6 1.7 1.8 Initially largely copied from: Yanofsky, Valerie R.; Mercer, Stephen E.; Phelps, Robert G. (2011). "Histopathological Variants of Cutaneous Squamous Cell Carcinoma: A Review
". Journal of Skin Cancer 2011: 1–13. doi:. ISSN 2090-2905.
-"This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited." - ↑ There are many variants for the processing of skin excisions. These examples use aspects from the following sources:
- . Handläggning av hudprover – provtagningsanvisningar, utskärningsprinciper och snittning (Handling of skin samples - sampling instructions, cutting principles and incision. Swedish Society of Pathology.
- For number of slices and coverage of lesions, depending on size. - Monica Dahlgren, Janne Malina, Anna Måsbäck, Otto Ljungberg. Stora utskärningen. KVAST (Swedish Society of Pathology). Retrieved on 2019-09-26.
- For slices towards the pointy ends to determine radicality, which can be parallel to the slices through the lesions (shown), or as longitudinal slices that go through each pointy end. - . Dermatopathology Grossing Guidelines. University of California, Los Angeles. Retrieved on 2019-10-23.
- For microtomy of the most central side at the lesion - "The principles of mohs micrographic surgery for cutaneous neoplasia
- With a "standard histologic examination" that, in addition to the lesion, only includes one section from each side along the longest diameter of the specimen.
- It also shows an example of circular coverage, with equal coverage distance in all four directions.
- The entire specimen may be submitted if the risk of malignancy is high. - . Handläggning av hudprover – provtagningsanvisningar, utskärningsprinciper och snittning (Handling of skin samples - sampling instructions, cutting principles and incision. Swedish Society of Pathology.
- ↑ Initially copied from: Paolino, Giovanni; Donati, Michele; Didona, Dario; Mercuri, Santo; Cantisani, Carmen (2017). "Histology of Non-Melanoma Skin Cancers: An Update
". Biomedicines 5 (4): 71. doi:. ISSN 2227-9059.
"This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/)."
Image sources