Difference between revisions of "Heart autopsy"
m (→Ruptured intercalated discs: of) |
(+Image) |
||
| Line 8: | Line 8: | ||
==Autopsy cutting checklist== | ==Autopsy cutting checklist== | ||
}} | }} | ||
| + | <gallery> | ||
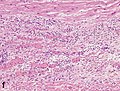
| + | File:Gross pathology of papillary muscle infarction.jpg|Circumferential slice of left ventricle, showing a fresh papillary muscle infarction. | ||
| + | </gallery> | ||
==Coronary arteries== | ==Coronary arteries== | ||
Revision as of 06:15, 30 December 2019
Author:
Mikael Häggström [note 1]
Autopsy of the heart:
Contents
Comprehensiveness
Factors supporting a relatively more comprehensive autopsy and/or report, particularly in the inclusion of negated findings:
- Lack of explanation from existing evidence. On the other hand, for example, upon finding an obvious aortic rupture, the rest of the autopsy is less relevant and may be relatively short.
- Double-reading: If your report is likely to undergo double reading by another pathologist before sign-out, it needs to be more detailed, because the doctor who will do the double-reading then knows that you have looked at those locations.
- Highly suspected locations, such as given from the referral.
On this resource, the following formatting is used for comprehensiveness:
- Minimal depth
- (Moderate depth)
- ((Comprehensive))
Autopsy cutting checklist
- Remove the parietal pericardium
- Separate the heart from the from lungs by cutting through the major vessels. The pulmonary artery should be cut first and the lumen inspected for any pulmonary embolism.
- Weigh the heart.
- Dissect the coronary vessels. More details in section below. Further information: Arteries
- On the right side of the heart, dissect in the direction of blood flow: Superior vena cava > right atrium > tricuspid valve > right ventricle. Look for thromboses or patent foramen ovale.[note 2]
- Dissect the atrial appendages, to exclude thromboses.
- Dissect the left ventricle, such as into circumferential slices from the apex to the base.[note 3] Inspect (and measure) the left ventricular wall thickness.

- (Measure the circumferences of the four valves. Cutoffs for valve dilatation:[1]
- Mitral valve: circumference greater than 9.9 cm in males and 9.1 cm in females
- Aortic valve: circumference greater than 8.5 cm in males and 7.9 cm in females
- Tricuspid valve: circumference greater than 11.8 cm in males and 11.1 cm in females
- Pulmonic valve: circumference greater than 7.5 cm in males and 7.4 cm in females)

Circumferential slice of left ventricle, showing a fresh papillary muscle infarction.

Coronary arteries

Make longitudinal (or transverse cuts at 3 mm intervals[2]) through:
- The right coronary artery.
- (The right marginal artery)
- The left coronary and circumflex artery.
- The left anterior descending artery.
- (The left marginal artery)
- (The left diagonal branch)
- Any vessel grafts to the heart
Estimate the percentage of any significant stenosis or occlusion.

Plaque at different percentages of atherosclerotic stenosis.[2]

The presence of a totally occlusive thrombotic mass confers a diagnosis of likely sudden cardiac death death even in the absence of microscopically visible necrosis.[2]
Myocardium
Look for:
- Signs of myocardial infarction:

Streched/wavy fibres

Coagulative necrosis: ‘hypereosinophilia’

Interstitial edema

Neutrophil karyorrhexis

Macrophages and lymphocytes
Vessel/endothelial sprouts

Fibroblast and young collagen

Dense fibrosis








If one or more is present, see Autopsy of myocardial infarction
- Ruptured intercalated discs (see section below)
Ruptured intercalated discs

Ruptured intercalated discs have two main causes:
- Microtome processing, thereby being a visual artifact,[3] not needing reporting.
- Forceful myocardial contraction, in turn mainly caused by ventricular fibrillation[4] or electric shock,[5]
Additional signs indicating forceful myocardial contraction, and thereby the mentioning of the findings in the report, are:[4][5]
- Alternating bundles of hypercontracted myocytes with hyperdistended ones.
- Square-shaped myocardiocyte nuclei.
- Hyperdistended myocardiocytes with detached sarcomeres, and in proximity of hypercontracted myocardiocytes.
Reporting
Example of a normal report:
- In the myocardium, there is no evidence of fresh lesion. No scar is seen. The myocardium has a homogeneous reddish brown color, without signs of postinfarction scarring or signs of acute infarction.
See also: General notes on reporting
Notes
- ↑ For a full list of contributors, see article history. Creators of images are attributed at the image description pages, seen by clicking on the images. See Patholines:Authorship for details.
- ↑ The right ventricle can alternatively be cut in circumferential slices along with the left ventricle.
- ↑ An alternative approach is to cut the left ventricle through a cut along the left lateral margin, followed by an anterior cut from the apex to the aortic root, freeing the anterior wall. Then cut through the plane of the myocardium of the anterior and posterior myocardial wall, as well as the septum, for any signs of infarction. (Dissect one or more papillary muscles for infarction.)
Main page
References
- ↑ Kitzman, Dalane W.; Scholz, David G.; Hagen, Philip T.; Ilstrup, Duane M.; Edwards, William D. (1988). "Age-Related Changes in Normal Human Hearts During the First 10 Decades of Life. Part II (Maturity): A Quantitative Anatomic Study of 765 Specimens From Subjects 20 to 99 Years Old
". Mayo Clinic Proceedings 63 (2): 137–146. doi:. ISSN 00256196.
- Griffith, Christopher C.; Raval, Jay S.; Nichols, Larry (2012). "Intravascular Talcosis due to Intravenous Drug Use Is an Underrecognized Cause of Pulmonary Hypertension
- ↑ 2.0 2.1 2.2 Michaud, Katarzyna; Basso, Cristina; d’Amati, Giulia; Giordano, Carla; Kholová, Ivana; Preston, Stephen D.; Rizzo, Stefania; Sabatasso, Sara; et al. (2019). "Diagnosis of myocardial infarction at autopsy: AECVP reappraisal in the light of the current clinical classification
". Virchows Archiv. doi:. ISSN 0945-6317.
- This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/)
- ↑ Page 38 in: Giorgio Baroldi (2004). The Etiopathogenesis of Coronary Heart Disease: A Heretical Theory Based on Morphology, Second Edition . CRC Press. ISBN 9781498712811.
- ↑ 4.0 4.1 Page 55 in: Vittorio Fineschi, Giorgio Baroldi, Malcolm D. Silver (2016). Pathology of the Heart and Sudden Death in Forensic Medicine . CRC Press. ISBN 9781420006438.
- ↑ 5.0 5.1 Fineschi, Vittorio; Karch, Steven B.; D'Errico, Stefano; Pomara, Cristoforo; Riezzo, Irene; Turillazzi, Emanuela (2005). "Cardiac pathology in death from electrocution ". International Journal of Legal Medicine 120 (2): 79–82. doi:. ISSN 0937-9827.
Image sources