Difference between revisions of "Heart autopsy"
(+Weight) |
(→Myocardium: Linked) |
||
| Line 56: | Line 56: | ||
File:Histopathology of granulation tissue with formation of microvessels in myocardial infarction.jpg|Vessel/endothelial sprouts | File:Histopathology of granulation tissue with formation of microvessels in myocardial infarction.jpg|Vessel/endothelial sprouts | ||
File:Histopathology of fibroblast proliferation and early collagen deposition in myocardial infarction.jpg|Fibroblast and young collagen | File:Histopathology of fibroblast proliferation and early collagen deposition in myocardial infarction.jpg|Fibroblast and young collagen | ||
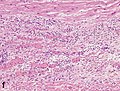
| − | File:Histopathology of dense fibrous scar replacing myocyte loss in myocardial infarction.jpg| | + | File:Histopathology of dense fibrous scar replacing myocyte loss in myocardial infarction.jpg|Fibrosis. {{further|Myocardial fibrosis|linebreak=no}} |
</gallery> | </gallery> | ||
If one or more is present, see '''[[Autopsy of myocardial infarction]]''' | If one or more is present, see '''[[Autopsy of myocardial infarction]]''' | ||
Revision as of 03:43, 31 January 2020
Author:
Mikael Häggström [note 1]
Autopsy of the heart:
Contents
Comprehensiveness
Factors supporting a relatively more comprehensive autopsy and/or report, particularly in the inclusion of negated findings:
- Lack of explanation from existing evidence. On the other hand, for example, upon finding an obvious aortic rupture, the rest of the autopsy is less relevant and may be relatively short.
- Double-reading: If your report is likely to undergo double reading by another pathologist before sign-out, it needs to be more detailed, because the doctor who will do the double-reading then knows that you have looked at those locations.
- Highly suspected locations, such as given from the referral.
On this resource, the following formatting is used for comprehensiveness:
- Minimal depth
- (Moderate depth)
- ((Comprehensive))
Autopsy cutting checklist
- Remove the parietal pericardium
- Separate the heart from the from lungs by cutting through the major vessels. The pulmonary artery should be cut first and the lumen inspected for any pulmonary embolism.
- Weigh the heart.
- Dissect the coronary vessels. More details in section below. Further information: Arteries
- On the right side of the heart, dissect in the direction of blood flow: Superior vena cava > right atrium > tricuspid valve > right ventricle. Look for thromboses or patent foramen ovale.[note 2]
- Dissect the atrial appendages, to exclude thromboses.
- Dissect the left ventricle, such as into circumferential slices from the apex to the base.[note 3] Inspect (and measure) the left ventricular wall thickness.

- (Measure the circumferences of the four valves. Cutoffs for valve dilatation:[1]
- Mitral valve: circumference greater than 9.9 cm in males and 9.1 cm in females
- Aortic valve: circumference greater than 8.5 cm in males and 7.9 cm in females
- Tricuspid valve: circumference greater than 11.8 cm in males and 11.1 cm in females
- Pulmonic valve: circumference greater than 7.5 cm in males and 7.4 cm in females)
| Mild | 12 to 13 mm |
| Moderate | >13 to 17 mm |
| Severe | >17 mm |
The average thickness of the left ventricle is up to 8 mm in women and 9 mm in men.[notes 1][3]

Circumferential slice of left ventricle, showing a fresh papillary muscle infarction.

Gross examination of coronary arteries

Make longitudinal (or transverse cuts at 3 mm intervals[4]) through:
- The right coronary artery.
- (The right marginal artery)
- The left coronary and circumflex artery.
- The left anterior descending artery.
- (The left marginal artery)
- (The left diagonal branch)
- Any vessel grafts to the heart
Estimate the percentage of any significant stenosis or occlusion.

Plaque at different percentages of atherosclerotic stenosis.[4]

The presence of a totally occlusive thrombotic mass confers a diagnosis of likely sudden cardiac death death even in the absence of microscopically visible necrosis.[4]
Weight
Cardiomegaly can be defined as a weight exceeding the 95th percentile of normal individuals, preferably adjusted for weight, size, age and gender.[5][notes 2]

Microscopic examination
Myocardium
Look for:
- Signs of myocardial infarction:

Streched/wavy fibres

Coagulative necrosis: ‘hypereosinophilia’

Interstitial edema

Neutrophil karyorrhexis

Macrophages and lymphocytes
Vessel/endothelial sprouts

Fibroblast and young collagen

Fibrosis. Further information: Myocardial fibrosis








If one or more is present, see Autopsy of myocardial infarction
- (Optionally, also look for:)

Ruptured intercalated discs. Further information: Ruptured intercalated discs

Reporting
This is en example report. In addition to comprehensiveness, it has the following annotations:
<< Decision needed between alternatives separated by / signs >>
{{Common findings / In case of findings}}
[[Comments]]
Organs or important regions are in bold in this example for clarity, but does not need to be in an actual report.
The heart << has normal weight / is enlarged [[ > 399 g in women and> 449 g in men]] >>, weighing ___ g. ((The epicardium is transparent. There is a moderate amount of subepicardial fat.
| Normal configuration | (No atrial or ventricular dilation. No ventricular wall thickening) / {{The left ventricle has {{concentric}} hypertrophy, with a wall thickness of ___ mm.}} | ((No atrial or ventricular dilation. The right and left auricular appendage is unremarkable. The left ventricular wall thickness is __ cm and the right is ___. The trabeculae carneae are normal ({[Finding-begin}}/ prominent /flattened}}.)) [[A comprehensive report may describe each atrium, valve and ventricle etc. in order of blood flow.]] |
(Foramen ovale is closed.) ((The ductus arteriosus is obliterated))
The coronary arteries ((arise in normal position. The coronary ostia are << patent {{partially occluded by arteriosclerotic calcification}}>>. They)) have << no / mild / moderate / severe >> {{and partially calcified}} arteriosclerosis. They are traced, ((throughout their length by transverse sections)) {{after fixation and decalcification}} <<without significant constrictions.{{ / The lumina of the left anterior descending, right coronary, and left circumflex coronary arteries are _%, _%, and _% narrowed, respectively.}} [[If the degree of stenosis on microscopy sections of coronary arteries only differ slightly from the gross description, preferably write "mild/moderate/severe atherosclerosis consistent with the gross inspection."]] (Gross measurement of coronary artery stenosis is generally more accurate than microscopic measurement, so the former generally has precedence.)
No thrombi in the cardiac atria (including auricles), chambers or coronary arteries.
| Chordae tendineae, the endocardium and heart valves are unremarkable. | (The endocardium is smooth and shiny. Chordae tendineae are unremarkable. The valves are normal in number, and are thin and fine at the openings.) | ((The endocardium is smooth, transparent and free of mural thrombi. The valve leaflets and chordae tendinae are overall delicate, pliable and free of lesion or calcification. <<Its leaflets are thin and pliable / No signs of inflammation>>.
{{The cusps are calcified at the bases / adherent to each other.}} {{The valve displays mild / moderate / severe myxomatous degeneration.}} The epicardium and subepicardium are unremarkable. The papillary muscles are normal {{ / hypertrophied}})) |
The myocardium has ((a homogeneous reddish brown color, and)) no signs of <<fresh lesion / ((areas of necrosis or hemorrhage))>> (or scar){{/ streaks of white scar tissue}}.
See also: General notes on reporting
Notes
- ↑ The numbers for the average thickness of the left ventricle are the 95% prediction interval for the short axis images at the mid-cavity level
- ↑ External link: Chicago model for post-mortem classification of cardiomegaly, adjusted for weight, size, age and gender.
- ↑ For a full list of contributors, see article history. Creators of images are attributed at the image description pages, seen by clicking on the images. See Patholines:Authorship for details.
- ↑ The right ventricle can alternatively be cut in circumferential slices along with the left ventricle.
- ↑ An alternative approach is to cut the left ventricle through a cut along the left lateral margin, followed by an anterior cut from the apex to the aortic root, freeing the anterior wall. Then cut through the plane of the myocardium of the anterior and posterior myocardial wall, as well as the septum, for any signs of infarction. (Dissect one or more papillary muscles for infarction.)
Main page
References
- ↑ Kitzman, Dalane W.; Scholz, David G.; Hagen, Philip T.; Ilstrup, Duane M.; Edwards, William D. (1988). "Age-Related Changes in Normal Human Hearts During the First 10 Decades of Life. Part II (Maturity): A Quantitative Anatomic Study of 765 Specimens From Subjects 20 to 99 Years Old
". Mayo Clinic Proceedings 63 (2): 137–146. doi:. ISSN 00256196.
- Griffith, Christopher C.; Raval, Jay S.; Nichols, Larry (2012). "Intravascular Talcosis due to Intravenous Drug Use Is an Underrecognized Cause of Pulmonary Hypertension
- ↑ Goland, Sorel; Czer, Lawrence S.C.; Kass, Robert M.; Siegel, Robert J.; Mirocha, James; De Robertis, Michele A.; Lee, Jason; Raissi, Sharo; et al. (2008). "Use of Cardiac Allografts With Mild and Moderate Left Ventricular Hypertrophy Can Be Safely Used in Heart Transplantation to Expand the Donor Pool ". Journal of the American College of Cardiology 51 (12): 1214–1220. doi:. ISSN 07351097.
- ↑ Kawel, Nadine; Turkbey, Evrim B.; Carr, J. Jeffrey; Eng, John; Gomes, Antoinette S.; Hundley, W. Gregory; Johnson, Craig; Masri, Sofia C.; et al. (2012). "Normal Left Ventricular Myocardial Thickness for Middle-Aged and Older Subjects With Steady-State Free Precession Cardiac Magnetic Resonance ". Circulation: Cardiovascular Imaging 5 (4): 500–508. doi:. ISSN 1941-9651.
- ↑ 4.0 4.1 4.2 Michaud, Katarzyna; Basso, Cristina; d’Amati, Giulia; Giordano, Carla; Kholová, Ivana; Preston, Stephen D.; Rizzo, Stefania; Sabatasso, Sara; et al. (2019). "Diagnosis of myocardial infarction at autopsy: AECVP reappraisal in the light of the current clinical classification
". Virchows Archiv. doi:. ISSN 0945-6317.
- This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/)
- ↑ . Chicago model for post-mortem classification of cardiomegaly. Northwestern University Feinberg School of Medicine. Retrieved on 2020-01-15.
- ↑ Kumar, Neena Theresa; Liestøl, Knut; Løberg, Else Marit; Reims, Henrik Mikael; Mæhlen, Jan (2014). "Postmortem heart weight: relation to body size and effects of cardiovascular disease and cancer ". Cardiovascular Pathology 23 (1): 5–11. doi:. ISSN 10548807.
Image sources