Difference between revisions of "Endometrial cancer"
(Format) |
(→Staging: +CK) |
||
| (12 intermediate revisions by the same user not shown) | |||
| Line 57: | Line 57: | ||
File:Histopathology of endometrial intraepithelial neoplasia (EIN).jpg|'''Endometrial intraepithelial neoplasia''' ('''EIN'''), for comparison, also showing gland crowding and atypia compared to normal endometrium, but without invasion.<ref name="OwingsQuick2014">{{cite journal|last1=Owings|first1=Richard A.|last2=Quick|first2=Charles M.|title=Endometrial Intraepithelial Neoplasia|journal=Archives of Pathology & Laboratory Medicine|volume=138|issue=4|year=2014|pages=484–491|issn=1543-2165|doi=10.5858/arpa.2012-0709-RA}}</ref> | File:Histopathology of endometrial intraepithelial neoplasia (EIN).jpg|'''Endometrial intraepithelial neoplasia''' ('''EIN'''), for comparison, also showing gland crowding and atypia compared to normal endometrium, but without invasion.<ref name="OwingsQuick2014">{{cite journal|last1=Owings|first1=Richard A.|last2=Quick|first2=Charles M.|title=Endometrial Intraepithelial Neoplasia|journal=Archives of Pathology & Laboratory Medicine|volume=138|issue=4|year=2014|pages=484–491|issn=1543-2165|doi=10.5858/arpa.2012-0709-RA}}</ref> | ||
File:Histopathology of serous carcinoma of uterus.jpg|'''Papillary serous carcinoma''' of uterus, with characteristic discohesiveness of cells (like falling apart) around fibrovascular cores.{{MH}} | File:Histopathology of serous carcinoma of uterus.jpg|'''Papillary serous carcinoma''' of uterus, with characteristic discohesiveness of cells (like falling apart) around fibrovascular cores.{{MH}} | ||
| − | File:Histopathology of papillary serous carcinoma of the endometrium.jpg|'''Papillary serous carcinoma''' of uterus, in this case showing both papillary and micropapillary architecture.<ref name=Murali2019/> | + | File:Histopathology of papillary serous carcinoma of the endometrium.jpg|'''Papillary serous carcinoma''' of uterus, in this case showing both papillary and micropapillary architecture.<ref name=Murali2019>{{cite journal| author=Rajmohan Murali, M.B.B.S., M.D., F.R.C.P.A., Ben Davidson, M.D., Ph.D., Oluwole Fadare, M.D., Joseph A. Carlson, M.D., Ph.D., Christopher P. Crum, M.D., C. Blake Gilks, M.D., Julie A. Irving, M.D., F.R.C.P.C., Anais Malpica, M.D., Xavier Matias-Guiu, M.D., Ph.D., W. Glenn McCluggage, F.R.C.Path., Khush Mittal, M.D., Esther Oliva, M.D., Vinita Parkash, M.D., Joanne K. L. Rutgers, M.D., Paul N. Staats, M.D., Colin J. R. Stewart, M.D., Carmen Tornos, M.D., and Robert A. Soslow, M.D. | title=High-grade Endometrial Carcinomas: Morphologic and Immunohistochemical Features, Diagnostic Challenges and Recommendations. | journal=Int J Gynecol Pathol | year= 2019 | volume= 38 Suppl 1 | issue= | pages= S40-S63 | pmid=30550483 | doi=10.1097/PGP.0000000000000491 | pmc=6296248 | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=30550483 }}<br>- "This is an open access article distributed under the Creative Commons Attribution License 4.0 (CCBY), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited."</ref> |
File:Histopathology of clear cell carcinoma of the endometrium with papillary architecture.png|'''Clear cell carcinoma''' of the endometrium with '''papillary''' architecture, characteristically small round papillae lacking overt stratification.<ref name=Murali2019/> Clear cell carcinoma is defined as a carcinoma demonstrating a combination of papillary, tubulocystic and/or solid architectural patterns, with cuboidal or polygonal cells containing nuclei with a variable pleomorphism (although usually lacking discernible pleomorphism).<ref name=Murali2019/> | File:Histopathology of clear cell carcinoma of the endometrium with papillary architecture.png|'''Clear cell carcinoma''' of the endometrium with '''papillary''' architecture, characteristically small round papillae lacking overt stratification.<ref name=Murali2019/> Clear cell carcinoma is defined as a carcinoma demonstrating a combination of papillary, tubulocystic and/or solid architectural patterns, with cuboidal or polygonal cells containing nuclei with a variable pleomorphism (although usually lacking discernible pleomorphism).<ref name=Murali2019/> | ||
File:Histopathology of clear cell carcinoma of the endometrium with tubulocystic architecture.png|'''Clear cell carcinoma''' of the endometrium with '''tubulocystic''' architecture.<ref name=Murali2019/> | File:Histopathology of clear cell carcinoma of the endometrium with tubulocystic architecture.png|'''Clear cell carcinoma''' of the endometrium with '''tubulocystic''' architecture.<ref name=Murali2019/> | ||
| Line 67: | Line 67: | ||
===Endometrioid adenocarcinoma=== | ===Endometrioid adenocarcinoma=== | ||
For endometrioid adenocarcinoma, perform '''architectural grading''':<ref name="SoslowTornos2019">{{cite journal|last1=Soslow|first1=Robert A.|last2=Tornos|first2=Carmen|last3=Park|first3=Kay J.|last4=Malpica|first4=Anais|last5=Matias-Guiu|first5=Xavier|last6=Oliva|first6=Esther|last7=Parkash|first7=Vinita|last8=Carlson|first8=Joseph|last9=McCluggage|first9=W. Glenn|last10=Gilks|first10=C. Blake|title=Endometrial Carcinoma Diagnosis|journal=International Journal of Gynecological Pathology|volume=38|year=2019|pages=S64–S74|issn=0277-1691|doi=10.1097/PGP.0000000000000518}}</ref> | For endometrioid adenocarcinoma, perform '''architectural grading''':<ref name="SoslowTornos2019">{{cite journal|last1=Soslow|first1=Robert A.|last2=Tornos|first2=Carmen|last3=Park|first3=Kay J.|last4=Malpica|first4=Anais|last5=Matias-Guiu|first5=Xavier|last6=Oliva|first6=Esther|last7=Parkash|first7=Vinita|last8=Carlson|first8=Joseph|last9=McCluggage|first9=W. Glenn|last10=Gilks|first10=C. Blake|title=Endometrial Carcinoma Diagnosis|journal=International Journal of Gynecological Pathology|volume=38|year=2019|pages=S64–S74|issn=0277-1691|doi=10.1097/PGP.0000000000000518}}</ref> | ||
| − | |||
| − | |||
| − | |||
| − | |||
| − | |||
<gallery mode="packed" heights="200"> | <gallery mode="packed" heights="200"> | ||
| − | File:Histopathology of | + | File:Histopathology of FIGO (architectural) grade 1 endometrial adenocarcinoma.png|'''Grade 1: ≤5%''' solid non-glandular, non-squamous growth.{{MH}} |
| − | File:Histopathology of grade 2 endometrioid endometrial adenocarcinoma with mucinous differentiation, low magnification.jpg|'''Grade 2''' | + | File:FIGO grade 2 endometrial adenocarcinoma.jpg|'''Grade 2: >5% and ≤50%''' solid non-glandular, non-squamous growth.{{MH}} |
| − | File: | + | File:Histopathology of grade 2 endometrioid endometrial adenocarcinoma with mucinous differentiation, low magnification.jpg|'''Grade 2''', with mucinous differentiation.<ref group=notes>Mucinous endometrioid adenocarcinoma is an altered differentiation / metaplasia with intracytoplasmic mucin (intraluminal mucin pooling does not qualify).<br>- {{cite web|url=http://www.pathologyoutlines.com/topic/uterusendometrioid.html|title=Uterus - Carcinoma - Endometrioid carcinoma|author=Aarti Sharma, M.D., Ricardo R. Lastra, M.D.|website=PathologyOutlines}} Topic Completed: 3 September 2020. Minor changes: 21 September 2020</ref> |
| − | + | File:FIGO grade 3 endometrial adenocarcinoma.jpg|'''Grade 3: >50%''' solid non-glandular, non-squamous growth.<ref name=Murali2019 group=image>{{cite journal| author=Rajmohan Murali, M.B.B.S., M.D., F.R.C.P.A., Ben Davidson, M.D., Ph.D., Oluwole Fadare, M.D., Joseph A. Carlson, M.D., Ph.D., Christopher P. Crum, M.D., C. Blake Gilks, M.D., Julie A. Irving, M.D., F.R.C.P.C., Anais Malpica, M.D., Xavier Matias-Guiu, M.D., Ph.D., W. Glenn McCluggage, F.R.C.Path., Khush Mittal, M.D., Esther Oliva, M.D., Vinita Parkash, M.D., Joanne K. L. Rutgers, M.D., Paul N. Staats, M.D., Colin J. R. Stewart, M.D., Carmen Tornos, M.D., and Robert A. Soslow, M.D. | title=High-grade Endometrial Carcinomas: Morphologic and Immunohistochemical Features, Diagnostic Challenges and Recommendations. | journal=Int J Gynecol Pathol | year= 2019 | volume= 38 Suppl 1 | issue= | pages= S40-S63 | pmid=30550483 | doi=10.1097/PGP.0000000000000491 | pmc=6296248 | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=30550483 }}<br>- "This is an open access article distributed under the Creative Commons Attribution License 4.0 (CCBY), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited."</ref> Carcinomas with identifiable endometrial component, and with over 50% solid architecture should be classified as grade 3 endometrioid carcinoma.<ref name=Murali2019/> | |
</gallery> | </gallery> | ||
:{{Moderate-begin}}Also perform '''nuclear grading:'''{{Moderate-end}} | :{{Moderate-begin}}Also perform '''nuclear grading:'''{{Moderate-end}} | ||
<gallery mode="packed" heights="200"> | <gallery mode="packed" heights="200"> | ||
| − | File:Histopathology of endometrioid cancer, grade 1, nuclear grade 1.jpg|'''Nuclear grade 1''': Oval, mildly enlarged nucleus with evenly distributed chromatin.{{MH}}<ref name= | + | File:Histopathology of endometrioid cancer, grade 1, nuclear grade 1.jpg|'''Nuclear grade 1''': Oval, mildly enlarged nucleus with evenly distributed chromatin.{{MH}}<ref name=Nofech-Mozes2012>Source for nuclear grade criteria:<br>- {{cite journal| author=Nofech-Mozes S, Ismiil N, Dubé V, Saad RS, Ghorab Z, Grin A | display-authors=etal| title=Interobserver agreement for endometrial cancer characteristics evaluated on biopsy material. | journal=Obstet Gynecol Int | year= 2012 | volume= 2012 | issue= | pages= 414086 | pmid=22496699 | doi=10.1155/2012/414086 | pmc=3306930 | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=22496699 }} </ref> |
| − | File:Histopathology of endometrioid cancer, grade 1, nuclear grade 2.jpg|'''Nuclear grade 2''': Intermediate features.{{MH}}<ref name= | + | File:Histopathology of endometrioid cancer, grade 1, nuclear grade 2.jpg|'''Nuclear grade 2''': Intermediate features.{{MH}}<ref name=Nofech-Mozes2012/> |
| + | File:Endometrial endometrioid adenocarcinoma, nuclear and architectural grade 3.jpg|'''Nuclear grade 3''': Markedly enlarged and pleomorphic nuclei, with coarse chromatin and distinct nucleoli.{{MH}}<ref name=Nofech-Mozes2012/> | ||
</gallery> | </gallery> | ||
| − | |||
| − | |||
====FIGO grading==== | ====FIGO grading==== | ||
Perform FIGO grading in case of endometrioid or mucinous carcinomas. FIGO classification is architectural grading as above, but that the presence of grade 3 nuclear atypia in an architectural pattern grade I tumor '''raises the grade by one point''':<ref name=who5th>{{cite book | author=World Health Organization. Classification of Tumours Editorial Board | author2=International Agency for Research on Cancer | author3=World Health Organization | title=Female genital tumours | publication-place=Lyon, France | date=2020 | isbn=978-92-832-4504-9 | oclc=1199943903 | language=nl}}</ref><ref name="pmid26715172">{{cite journal| author=Malpica A| title=How to approach the many faces of endometrioid carcinoma. | journal=Mod Pathol | year= 2016 | volume= 29 Suppl 1 | issue= | pages= S29-44 | pmid=26715172 | doi=10.1038/modpathol.2015.142 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=26715172 }} </ref> | Perform FIGO grading in case of endometrioid or mucinous carcinomas. FIGO classification is architectural grading as above, but that the presence of grade 3 nuclear atypia in an architectural pattern grade I tumor '''raises the grade by one point''':<ref name=who5th>{{cite book | author=World Health Organization. Classification of Tumours Editorial Board | author2=International Agency for Research on Cancer | author3=World Health Organization | title=Female genital tumours | publication-place=Lyon, France | date=2020 | isbn=978-92-832-4504-9 | oclc=1199943903 | language=nl}}</ref><ref name="pmid26715172">{{cite journal| author=Malpica A| title=How to approach the many faces of endometrioid carcinoma. | journal=Mod Pathol | year= 2016 | volume= 29 Suppl 1 | issue= | pages= S29-44 | pmid=26715172 | doi=10.1038/modpathol.2015.142 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=26715172 }} </ref> | ||
| Line 183: | Line 177: | ||
File:Histopathology of grade 2 endometrioid endometrial cancer with myometrial invasion.jpg|For biopsies, just look for absence or presence of myometrial invasion (pictured). | File:Histopathology of grade 2 endometrioid endometrial cancer with myometrial invasion.jpg|For biopsies, just look for absence or presence of myometrial invasion (pictured). | ||
File:Histopathology of endometrial cancer with lymphovascular invasion.jpg|Generally look for '''lymphovascular invasion''' (pictured) as well. | File:Histopathology of endometrial cancer with lymphovascular invasion.jpg|Generally look for '''lymphovascular invasion''' (pictured) as well. | ||
| + | File:HE histopathology and CK AE1-AE3 immunohistochemistry in endometrial adenocarcinoma metastasis to lymph node.png|For '''pelvic lymph nodes''', minor metastasis of endometrial cancer is hard to see (left panel). Therefore, if not obviously present, perform immunohistochemistry for CK AE1/AE3 (middle panel), and correlate positive findings with adenocarcinoma on high magnification (right panel). | ||
</gallery> | </gallery> | ||
| Line 196: | Line 191: | ||
| | | | ||
[[File:Patterns of p53 expression.png|right|420px]] | [[File:Patterns of p53 expression.png|right|420px]] | ||
| − | This image shows different patterns of '''p53 expression''' in endometrial cancers on [[immunohistochemistry]], whereof all except wild-type are variably termed abnormal/aberrant/mutation-type and are strongly predictive of an underlying p53 mutation | + | This image shows different patterns of '''p53 expression''' in endometrial cancers on [[immunohistochemistry]], whereof all except wild-type are variably termed abnormal/aberrant/mutation-type and are strongly predictive of an underlying p53 mutation, and correlates with higher grade carcinoma.<ref>{{cite journal| author=Köbel M, Ronnett BM, Singh N, Soslow RA, Gilks CB, McCluggage WG| title=Interpretation of P53 Immunohistochemistry in Endometrial Carcinomas: Toward Increased Reproducibility. | journal=Int J Gynecol Pathol | year= 2019 | volume= 38 Suppl 1 | issue= | pages= S123-S131 | pmid=29517499 | doi=10.1097/PGP.0000000000000488 | pmc=6127005 | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=29517499 }}<br>- "This is an open access article distributed under the Creative Commons Attribution License 4.0"</ref> |
| − | *'''Wild-type''', upper left: | + | *'''Wild-type''' expression, upper left: Variable proportion of tumor cell nuclei staining with variable intensity. This pattern should not be reported as “positive,” because this is ambiguous reporting language. |
| − | *'''Overexpression''', upper right: | + | *'''Overexpression''', upper right: Showing strong staining in virtually all tumor cell nuclei (as can be compared with the internal control of fibroblasts in the center). There is some cytoplasmic background indicating that this staining is quite strong but this should not be interpreted as abnormal cytoplasmic pattern. |
| − | *'''Complete absence''', lower left | + | *'''Complete absence''' of expression, lower left. In comparison, there wild-type pattern in normal atrophic glands at 12 and 6 o’clock. |
| − | *'''Both cytoplasmic and nuclear''', lower right | + | *'''Both cytoplasmic and nuclear''' expression, lower right. This case has similar intensity of the two, whereas stroma and normal endometrial glands show nuclear wild-type pattern. |
|} | |} | ||
===Microscopy report=== | ===Microscopy report=== | ||
| − | Example: | + | Example for a '''polypectomy''': |
{| class="wikitable" | {| class="wikitable" | ||
| − | | | + | | {{Moderate-begin}}Endometrium, polypectomy:{{Moderate-end}}<br> Endometrial adenocarcinoma, endometrioid type, FIGO grade 2, {{Moderate-begin}}nuclear grade 2{{Moderate-end}} with mucinous differentiation. Carcinoma focally invades myometrial smooth muscle. |
<gallery mode="packed"> | <gallery mode="packed"> | ||
| Line 214: | Line 209: | ||
</gallery> | </gallery> | ||
|} | |} | ||
| − | {{CAP}}<noinclude> | + | |
| + | Example for a '''hysterectomy''': | ||
| + | {|class=wikitable | ||
| + | | A. Uterus, cervix, bilateral {{Moderate-begin}}fallopian{{Moderate-end}} tubes and ovaries, hysterectomy and bilateral salpingo-oophorectomy: | ||
| + | *{{Moderate-begin}}Endometrial{{Moderate-end}} endometrioid adenocarcinoma FIGO grade 1, {{Moderate-begin}}nuclear grade 2{{Moderate-end}}. | ||
| + | *Carcinoma invades 40% of the myometrial thickness. | ||
| + | *Involvement of the lower uterine segment is present. | ||
| + | *Benign cervix | ||
| + | *Benign {{Moderate-begin}}fallopian{{Moderate-end}} tubes and ovaries. | ||
| + | *See synoptic report {{Finding-begin}}and comment{{Finding-end}}. | ||
| + | |||
| + | B. Left pelvic sentinel lymph nodes, excision: | ||
| + | *Three {{Moderate-begin}}(0/3){{Moderate-end}} benign lymph nodes{{Moderate-begin}}, negative for metastatic carcinoma on H&E and cytokeratin AE1/AE3 stains.{{Moderate-end}} | ||
| + | |||
| + | C. Right pelvic lymph nodes, excision: | ||
| + | *Two {{Moderate-begin}}(0/2){{Moderate-end}} benign lymph nodes{{Moderate-begin}}, negative for metastatic carcinoma.{{Moderate-end}} | ||
| + | |} | ||
| + | {{CAP}} Example, following the hysterectomy above: | ||
| + | {|class=wikitable | ||
| + | SYNOPTIC REPORT: | ||
| + | *Procedure: Total hysterectomy and bilateral salpingo-oophorectomy | ||
| + | *Tumor Site: Endometrium | ||
| + | *Tumor Size: 5.3 centimeters (cm) | ||
| + | *Histologic Type: Endometrioid carcinoma, NOS | ||
| + | *Histologic Grade: FIGO grade 1 | ||
| + | *Two-Tier Grading System: Low grade (encompassing FIGO 1 and 2) | ||
| + | *Myometrial Invasion: Present | ||
| + | *Depth of Myometrial Invasion: 10 mm | ||
| + | *Myometrial Thickness: 25 mm | ||
| + | *Percentage of Myometrial Invasion 40% | ||
| + | *Adenomyosis: Present, uninvolved by carcinoma | ||
| + | *Uterine serosa involvement: Not identified | ||
| + | *Lower uterine segment involvement: Present, superficial (non-myoinvasive) | ||
| + | *Cervical stromal involvement: Not identified | ||
| + | *Other tissue/organ involvement: Not identified | ||
| + | *Peritoneal/ascitic fluid: Not submitted / unknown | ||
| + | *Lymphovascular invasion (LVI): Not identified | ||
| + | *Margin Status: All margins negative for invasive carcinoma | ||
| + | *Regional lymph nodes | ||
| + | :*Regional lymph node status: All regional lymph nodes negative for tumor cells | ||
| + | :*Total number of pelvic nodes examined: 5 | ||
| + | :*Number of pelvic sentinel nodes examined: 3 | ||
| + | :*Total number of para-aortic nodes examined: 0 | ||
| + | :*Number of Para-aortic Sentinel Nodes Examined: 0 | ||
| + | *Pathologic Stage Classification (pTNM, AJCC 8th Edition) | ||
| + | :*pT Category: pT1a | ||
| + | :*pN Category: pN0 | ||
| + | *Additional Findings: leiomyomas | ||
| + | |||
| + | Results of immunohistochemical testing for mismatch repair (mmr) proteins, performed on block "A5": | ||
| + | *MLH-1: Intact nuclear expression | ||
| + | *PMS-2: Intact nuclear expression | ||
| + | *MSH-2: Intact nuclear expression | ||
| + | *SSH-6: Intact nuclear expression | ||
| + | |} | ||
| + | <noinclude> | ||
{{Bottom}} | {{Bottom}} | ||
</noinclude> | </noinclude> | ||
Latest revision as of 14:43, 10 December 2023
Author:
Mikael Häggström [note 1]
Contents
Presentations
Comprehensiveness
On this resource, the following formatting is used for comprehensiveness:
- Minimal depth
- (Moderate depth)
- ((Comprehensive))
Gross processing

A regular hysterectomy grossing is performed, but with the following sampling and additions:[1]
- 2 longitudinal sections through ecto/endocervix (1 anterior and 1 posterior).
- 2 longitudinal sections through upper endocervix/lower uterine segment (1 anterior and 1 posterior), contiguous with sections taken from cervix.
- Tumor:
- Measure greatest dimension of tumor.
- If tumor is smaller than 3 cm, submit entirely.
- If tumor is larger than 3 cm, submit 1 per cm.

- Measure tumor thickness and entire thickness of the wall, at the location of greatest percentage of tumor relative to wall thickness.
- Include 2 full-thickness sections (1 anterior and 1 posterior) at locations with seemingly greatest invasion. It may need multiple contiguous sections.
- Remaining sections can be superficial to include tumor and inner myometrium, such as from lower uterine segment to fundus to maintain orientation.
- If possible, include 1 section with interface between tumor and normal.
- Sections of any additional pathology, such as leiomyomas, polyps in their entirety.
- 1 section of uninvolved endometrium if present.
- Inspect serosa for implants and submit sections if grossly detected.
- For serous carcinomas, submit the entire ovary and fallopian tube:
- Ovary, serially sectioned perpendicular to long axis.
- SEE-FIM protocol for fallopian tubes:
- Remove the distal 2 cm (fimbriae) and section it parallel to the long axis.
- Section the remainder of the tube transversely at 2-3 mm intervals.
- For all other cancer types, submit adnexa as follows:
- Ovaries: 2 representative sections of each.
- Fallopian tubes: Entire fimbriae (longitudinally sectioned) and 2 representative cross-sections on each side.
- Size smaller than 2 mm: submit intact.
- Size larger than 2 mm: serially section perpendicular to the long axis in 2 mm intervals.
- If no gross tumor, submit entirely.
- If grossly positive, submit 1-2 representative sections showing the greatest tumor dimension and extranodal fat.
Microscopic evaluation
Diagnosis

Relative incidences of endometrial carcinomas by histopathology, being endometrioid in a majority of cases.[2] Endometrioid carcinoma has patterns reminiscent of normal endometrium, with many new glands formed from columnar epithelium with some abnormal nuclei:

Endometrial intraepithelial neoplasia (EIN), for comparison, also showing gland crowding and atypia compared to normal endometrium, but without invasion.[5]

Papillary serous carcinoma of uterus, with characteristic discohesiveness of cells (like falling apart) around fibrovascular cores.[image 1]

Papillary serous carcinoma of uterus, in this case showing both papillary and micropapillary architecture.[6]

Clear cell carcinoma of the endometrium with papillary architecture, characteristically small round papillae lacking overt stratification.[6] Clear cell carcinoma is defined as a carcinoma demonstrating a combination of papillary, tubulocystic and/or solid architectural patterns, with cuboidal or polygonal cells containing nuclei with a variable pleomorphism (although usually lacking discernible pleomorphism).[6]

Clear cell carcinoma of the endometrium with tubulocystic architecture.[6]

Clear cell carcinoma of the endometrium with solid architecture.[6]

Dedifferantiated carcinoma, a tumor that contains a component of undifferentiated endometrial carcinoma (UEC) and a component of conventional, usually lower-grade, endometrioid adenocarcinoma.[6]

Carcinosarcoma of the endometrium, with carcinoma in addition to sarcoma (seen here as atypical fibrovascular cores).[6]

_endometrial_endometrioid_adenocarcinoma.png)
.jpg)




Endometrioid adenocarcinoma
For endometrioid adenocarcinoma, perform architectural grading:[7]

Grade 1: ≤5% solid non-glandular, non-squamous growth.[image 1]

Grade 2: >5% and ≤50% solid non-glandular, non-squamous growth.[image 1]

Grade 2, with mucinous differentiation.[notes 1]
_grade_1_endometrial_adenocarcinoma.png)



- (Also perform nuclear grading:)
FIGO grading
Perform FIGO grading in case of endometrioid or mucinous carcinomas. FIGO classification is architectural grading as above, but that the presence of grade 3 nuclear atypia in an architectural pattern grade I tumor raises the grade by one point:[9][10]
- FIGO grade 1: ≤5% solid non-glandular, non-squamous growth
- FIGO grade 2:
- >5% and ≤50% solid non-glandular, non-squamous growth
- or
- ≤5% solid non-glandular, non-squamous growth and markedly enlarged and pleomorphic nuclei, with coarse chromatin and distinct nucleoli (in these cases, also consider a serous carcinoma of glandular variant)
- FIGO grade 3: >50% solid non-glandular, non-squamous growth
Bimodal grading
It is recommended to classify FIGO grade 1 and 2 tumors as low-grade, and grade 3 tumors as high-grade.[9]
Staging
Preferably, stage by both the AJCC TNM system and the FIGO system:[11] The following system is for uterine carcinoma and carcinosarcoma (but a separate staging system is used for sarcomas).
| T Category | FIGO Stage | T Criteria |
|---|---|---|
| TX | Primary tumor cannot be assessed | |
| T0 | No evidence of primary tumor | |
| T1 | I | Tumor confined to the corpus uteri, including endocervical glandular involvement |
| T1a | IA | Tumor limited to the endometrium or invading less than half the myometrium |
| T1b | IB | Tumor invading one half or more of the myometrium |
| T2 | II | Tumor invading the stromal connective tissue of the cervix but not extending beyond the uterus. Does NOT include endocervical glandular involvement. |
| T3 | III | Tumor involving serosa, adnexa, vagina, or parametrium |
| T3a | IIIA | Tumor involving the serosa and/or adnexa (direct extension or metastasis) |
| T3b | IIIB | Vaginal involvement (direct extension or metastasis) or parametrial involvement |
| T4 | IVA | Tumor invading the bladder mucosa and/or bowel mucosa (bullous edema is not sufficient to classify a tumor as T4) |
| N Category | FIGO Stage | N Criteria |
|---|---|---|
| NX | Regional lymph nodes cannot be assessed | |
| N0 | No regional lymph node metastasis | |
| N0(i+) | Isolated tumor cells in regional lymph node(s) no greater than 0.2 mm | |
| N1 | IIIC1 | Regional lymph node metastasis to pelvic lymph nodes |
| N1mi | IIIC1 | Regional lymph node metastasis (greater than 0.2 mm but not greater than 2.0 mm in diameter) to pelvic lymph nodes |
| N1a | IIIC1 | Regional lymph node metastasis (greater than 2.0 mm in diameter) to pelvic lymph nodes |
| N2 | IIIC2 | Regional lymph node metastasis to para-aortic lymph nodes, with or without positive pelvic lymph nodes |
| N2mi | IIIC2 | Regional lymph node metastasis (greater than 0.2 mm but not greater than 2.0 mm in diameter) to para-aortic lymph nodes, with or without positive pelvic lymph nodes |
| N2a | IIIC2 | Regional lymph node metastasis (greater than 2.0 mm in diameter) to para-aortic lymph nodes, with or without positive pelvic lymph nodes |
The suffix (sn) is added to the N category when metastasis is identified only by sentinel lymph node biopsy.
| M Category | FIGO Stage | M Criteria |
|---|---|---|
| M0 | No distant metastasis | |
| M1 | IVB | Distant metastasis (includes metastasis to inguinal lymph nodes, intraperitoneal disease, lung, liver, or bone). (It excludes metastasis to pelvic or para-aortic lymph nodes, vagina, uterine serosa, or adnexa). |
- AJCC Prognostic Stage Groups
| When T is… | And N is… | And M is… | Then the stage group is… |
|---|---|---|---|
| T1 | N0 | M0 | I |
| T1a | N0 | M0 | IA |
| T1b | N0 | M0 | IB |
| T2 | N0 | M0 | II |
| T3 | N0 | M0 | III |
| T3a | N0 | M0 | IIIA |
| T3b | N0 | M0 | IIIB |
| T1-T3 | N1/N1mi/N1a | M0 | IIIC1 |
| T1-T3 | N2/N2mi/N2a | M0 | IIIC2 |
| T4 | Any N | M0 | IVA |
| Any T | Any N | M1 | IVB |
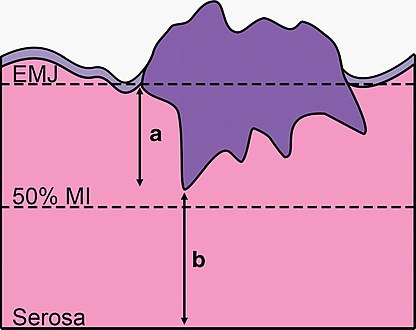
Calculation of myometrial invasion: The dotted lines show the position of the endometrial/myometrial junction (EMJ), and the line where the tumor would invade half of the myometrium (50 % MI). The arrows show the absolute depth of invasion (a) and tumor-free distance (b) measurements. Invasion as a percentage is calculated as:
a / (a+b)
For biopsies, just look for absence or presence of myometrial invasion (pictured).

Generally look for lymphovascular invasion (pictured) as well.

For pelvic lymph nodes, minor metastasis of endometrial cancer is hard to see (left panel). Therefore, if not obviously present, perform immunohistochemistry for CK AE1/AE3 (middle panel), and correlate positive findings with adenocarcinoma on high magnification (right panel).




Further workup
Generally perform the following molecular testing on endometrial carcinomas:[12]
- Mismatch repair (MMR) genes (MLH-1, PMS-2, MSH-2 and MSH-6) on all cancer types and grades. If MLH1 is lost, test for MLH1 promotor methylation.
- ER/PR and p53 for all high grade carcinomas regardless of stage.
- HER2 on all high grade carcinomas, or only on serous carcinomas, or those that are stage III or IV or recurrent.
For MMR genes, scoring is as follows:[13]

0% nuclear expression in tumor cell nuclei: Loss of expression (expression seen in stromal cells in image)

More than 0% but less than 10%: Indeterminate expression

10% or more: Retained expression



 This image shows different patterns of p53 expression in endometrial cancers on immunohistochemistry, whereof all except wild-type are variably termed abnormal/aberrant/mutation-type and are strongly predictive of an underlying p53 mutation, and correlates with higher grade carcinoma.[14]
|
Microscopy report
Example for a polypectomy:
| (Endometrium, polypectomy:) Endometrial adenocarcinoma, endometrioid type, FIGO grade 2, (nuclear grade 2) with mucinous differentiation. Carcinoma focally invades myometrial smooth muscle. |

Example for a hysterectomy:
A. Uterus, cervix, bilateral (fallopian) tubes and ovaries, hysterectomy and bilateral salpingo-oophorectomy:
B. Left pelvic sentinel lymph nodes, excision:
C. Right pelvic lymph nodes, excision:
|
For cancers, generally include a synoptic report, such as per College of American Pathologists (CAP) protocols at cap.org/protocols-and-guidelines. Example, following the hysterectomy above:
SYNOPTIC REPORT:- Procedure: Total hysterectomy and bilateral salpingo-oophorectomy
- Tumor Site: Endometrium
- Tumor Size: 5.3 centimeters (cm)
- Histologic Type: Endometrioid carcinoma, NOS
- Histologic Grade: FIGO grade 1
- Two-Tier Grading System: Low grade (encompassing FIGO 1 and 2)
- Myometrial Invasion: Present
- Depth of Myometrial Invasion: 10 mm
- Myometrial Thickness: 25 mm
- Percentage of Myometrial Invasion 40%
- Adenomyosis: Present, uninvolved by carcinoma
- Uterine serosa involvement: Not identified
- Lower uterine segment involvement: Present, superficial (non-myoinvasive)
- Cervical stromal involvement: Not identified
- Other tissue/organ involvement: Not identified
- Peritoneal/ascitic fluid: Not submitted / unknown
- Lymphovascular invasion (LVI): Not identified
- Margin Status: All margins negative for invasive carcinoma
- Regional lymph nodes
- Regional lymph node status: All regional lymph nodes negative for tumor cells
- Total number of pelvic nodes examined: 5
- Number of pelvic sentinel nodes examined: 3
- Total number of para-aortic nodes examined: 0
- Number of Para-aortic Sentinel Nodes Examined: 0
- Pathologic Stage Classification (pTNM, AJCC 8th Edition)
- pT Category: pT1a
- pN Category: pN0
- Additional Findings: leiomyomas
- MLH-1: Intact nuclear expression
- PMS-2: Intact nuclear expression
- MSH-2: Intact nuclear expression
- SSH-6: Intact nuclear expression
Notes
- ↑ Mucinous endometrioid adenocarcinoma is an altered differentiation / metaplasia with intracytoplasmic mucin (intraluminal mucin pooling does not qualify).
- Aarti Sharma, M.D., Ricardo R. Lastra, M.D.. Uterus - Carcinoma - Endometrioid carcinoma. PathologyOutlines. Topic Completed: 3 September 2020. Minor changes: 21 September 2020
- ↑ For a full list of contributors, see article history. Creators of images are attributed at the image description pages, seen by clicking on the images. See Patholines:Authorship for details.
Main page
References
- ↑ Nicole Cipriani (2020-06-22). Gross Pathology Manual - Uterus, Endometrial Cancer. The University of Chicago Department of Pathology.
- ↑ Mendivil, Alberto; Schuler, Kevin M.; Gehrig, Paola A. (2009). "Non-Endometrioid Adenocarcinoma of the Uterine Corpus: A Review of Selected Histological Subtypes ". Cancer Control 16 (1): 46–52. doi:. ISSN 1073-2748.
- ↑ Stewart, Colin J.R.; Crum, Christopher P.; McCluggage, W. Glenn; Park, Kay J.; Rutgers, Joanne K.; Oliva, Esther; Malpica, Anais; Parkash, Vinita; et al. (2019). "Guidelines to Aid in the Distinction of Endometrial and Endocervical Carcinomas, and the Distinction of Independent Primary Carcinomas of the Endometrium and Adnexa From Metastatic Spread Between These and Other Sites
". International Journal of Gynecological Pathology 38: S75–S92. doi:. ISSN 0277-1691.
- "Figures - available via license: Creative Commons Attribution 4.0 International" - ↑ Rabban, Joseph T.; Gilks, C. Blake; Malpica, Anais; Matias-Guiu, Xavier; Mittal, Khush; Mutter, George L.; Oliva, Esther; Parkash, Vinita; et al. (2019). "Issues in the Differential Diagnosis of Uterine Low-grade Endometrioid Carcinoma, Including Mixed Endometrial Carcinomas ". International Journal of Gynecological Pathology 38: S25–S39. doi:. ISSN 0277-1691.
- ↑ Owings, Richard A.; Quick, Charles M. (2014). "Endometrial Intraepithelial Neoplasia ". Archives of Pathology & Laboratory Medicine 138 (4): 484–491. doi:. ISSN 1543-2165.
- ↑ 6.0 6.1 6.2 6.3 6.4 6.5 6.6 6.7 Rajmohan Murali, M.B.B.S., M.D., F.R.C.P.A., Ben Davidson, M.D., Ph.D., Oluwole Fadare, M.D., Joseph A. Carlson, M.D., Ph.D., Christopher P. Crum, M.D., C. Blake Gilks, M.D., Julie A. Irving, M.D., F.R.C.P.C., Anais Malpica, M.D., Xavier Matias-Guiu, M.D., Ph.D., W. Glenn McCluggage, F.R.C.Path., Khush Mittal, M.D., Esther Oliva, M.D., Vinita Parkash, M.D., Joanne K. L. Rutgers, M.D., Paul N. Staats, M.D., Colin J. R. Stewart, M.D., Carmen Tornos, M.D., and Robert A. Soslow, M.D. (2019). "High-grade Endometrial Carcinomas: Morphologic and Immunohistochemical Features, Diagnostic Challenges and Recommendations.
". Int J Gynecol Pathol 38 Suppl 1: S40-S63. doi:. PMID 30550483. PMC: 6296248. Archived from the original. .
- "This is an open access article distributed under the Creative Commons Attribution License 4.0 (CCBY), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited." - ↑ Soslow, Robert A.; Tornos, Carmen; Park, Kay J.; Malpica, Anais; Matias-Guiu, Xavier; Oliva, Esther; Parkash, Vinita; Carlson, Joseph; et al. (2019). "Endometrial Carcinoma Diagnosis ". International Journal of Gynecological Pathology 38: S64–S74. doi:. ISSN 0277-1691.
- ↑ 8.0 8.1 8.2 Source for nuclear grade criteria:
- Nofech-Mozes S, Ismiil N, Dubé V, Saad RS, Ghorab Z, Grin A (2012). "Interobserver agreement for endometrial cancer characteristics evaluated on biopsy material. ". Obstet Gynecol Int 2012: 414086. doi:. PMID 22496699. PMC: 3306930. Archived from the original. . - ↑ 9.0 9.1 World Health Organization. Classification of Tumours Editorial Board; International Agency for Research on Cancer; World Health Organization (2020) (in nl). Female genital tumours . Lyon, France. ISBN 978-92-832-4504-9. OCLC 1199943903.
- ↑ Malpica A (2016). "How to approach the many faces of endometrioid carcinoma. ". Mod Pathol 29 Suppl 1: S29-44. doi:. PMID 26715172. Archived from the original. .
- ↑ Amin, Mahul (2017). AJCC cancer staging manual
(8 ed.). Switzerland: Springer. ISBN 978-3-319-40617-6. OCLC 961218414.
- For access, see the Secrets chapter of Patholines.
- Copyright note: The AJCC, 8th Ed. is published by a company in Switzerland, and the tables presented therein are Public Domain because they consist of tabular information without literary or artistic innovation, and therefore do not fulfil the inclusion criterion of the Swiss Copyright Act (CopA) which applies to "literary and artistic intellectual creations with individual character" (see Federal Act on Copyright and Related Rights (Copyright Act, CopA) of 9 October 1992 (Status as of 1 January 2022)). - ↑ Practice at Danbury Hospital, Danbury, Connecticut, New England.
- ↑ These cutoffs are used for both colorectal and endometrial cancers:
- Sarode, Venetia R.; Robinson, Linda (2019). "Screening for Lynch Syndrome by Immunohistochemistry of Mismatch Repair Proteins: Significance of Indeterminate Result and Correlation With Mutational Studies ". Archives of Pathology & Laboratory Medicine 143 (10): 1225–1233. doi:. ISSN 0003-9985.
- Sarode VR, Robinson L (2019). "Screening for Lynch Syndrome by Immunohistochemistry of Mismatch Repair Proteins: Significance of Indeterminate Result and Correlation With Mutational Studies. ". Arch Pathol Lab Med 143 (10): 1225-1233. doi:. PMID 30917047. Archived from the original. .
- Lee JHS, Li JJX, Chow C, Chan RCK, Kwan JSH, Lau TS (2021). "Long-Term Survival and Clinicopathological Implications of DNA Mismatch Repair Status in Endometrioid Endometrial Cancers in Hong Kong Chinese Women. ". Biomedicines 9 (10). doi:. PMID 34680502. PMC: 8533409. Archived from the original. . - ↑ Köbel M, Ronnett BM, Singh N, Soslow RA, Gilks CB, McCluggage WG (2019). "Interpretation of P53 Immunohistochemistry in Endometrial Carcinomas: Toward Increased Reproducibility.
". Int J Gynecol Pathol 38 Suppl 1: S123-S131. doi:. PMID 29517499. PMC: 6127005. Archived from the original. .
- "This is an open access article distributed under the Creative Commons Attribution License 4.0"
Image sources
- ↑ 1.0 1.1 1.2 1.3 1.4 1.5 Image(s) by: Mikael Häggström, M.D. Public Domain
- Author info
- Reusing images - ↑ Rajmohan Murali, M.B.B.S., M.D., F.R.C.P.A., Ben Davidson, M.D., Ph.D., Oluwole Fadare, M.D., Joseph A. Carlson, M.D., Ph.D., Christopher P. Crum, M.D., C. Blake Gilks, M.D., Julie A. Irving, M.D., F.R.C.P.C., Anais Malpica, M.D., Xavier Matias-Guiu, M.D., Ph.D., W. Glenn McCluggage, F.R.C.Path., Khush Mittal, M.D., Esther Oliva, M.D., Vinita Parkash, M.D., Joanne K. L. Rutgers, M.D., Paul N. Staats, M.D., Colin J. R. Stewart, M.D., Carmen Tornos, M.D., and Robert A. Soslow, M.D. (2019). "High-grade Endometrial Carcinomas: Morphologic and Immunohistochemical Features, Diagnostic Challenges and Recommendations.
". Int J Gynecol Pathol 38 Suppl 1: S40-S63. doi:. PMID 30550483. PMC: 6296248. Archived from the original. .
- "This is an open access article distributed under the Creative Commons Attribution License 4.0 (CCBY), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited."