Difference between revisions of "Evaluation"
m (→Artifacts: delinked) |
(Condenser) |
||
| (One intermediate revision by the same user not shown) | |||
| Line 5: | Line 5: | ||
[[File:Position of objective (edited).jpg|thumb|210px|Example starting position of objective.]] | [[File:Position of objective (edited).jpg|thumb|210px|Example starting position of objective.]] | ||
[[File:Microscopy slide scanning.jpg|thumb|Example slide scanning directions.]] | [[File:Microscopy slide scanning.jpg|thumb|Example slide scanning directions.]] | ||
| − | * | + | *Preferably, look up past '''medical history''' of the patient, mainly past cancers that could possibly appear in the current specimen. |
| + | *Look at each microscopy slide by '''eye''', to plan the microscopy screening so as to not miss peripheral fragments. | ||
*Have a systematic '''direction''' of screening through microscopy slides, such as from top left to bottom right as seen in the microscope. When two-way mirrored, the starting position of the microscope slide is then with the objective pointing at bottom right. | *Have a systematic '''direction''' of screening through microscopy slides, such as from top left to bottom right as seen in the microscope. When two-way mirrored, the starting position of the microscope slide is then with the objective pointing at bottom right. | ||
| + | |||
| + | ==Condenser== | ||
| + | Generally the condenser is placed in its highest position or just slightly lower. At low magnification objectives (mainly 4x and 10x objectives), the opening of the condenser (or iris) diaphragm should be wide open. For high-dry (40x) and oil-immersion objectives (100x), the diaphragm should be closed slowly while looking at a sharply focused section until the level of illumination is just slightly reduced, in order to attain optimal contrast and resolution.<ref>{{cite web|url=https://histologylab.ctl.columbia.edu/HistologyLabManual.pdf|title=Histology Laboratory Manual, Vagelos College of Physicians & Surgeons Columbia University|author=Patrice F Spitalnik|accessdate=2021-09-20}}</ref> | ||
==Artifacts== | ==Artifacts== | ||
Revision as of 13:53, 20 September 2021
Author:
Mikael Häggström [note 1]
.jpg)

- Preferably, look up past medical history of the patient, mainly past cancers that could possibly appear in the current specimen.
- Look at each microscopy slide by eye, to plan the microscopy screening so as to not miss peripheral fragments.
- Have a systematic direction of screening through microscopy slides, such as from top left to bottom right as seen in the microscope. When two-way mirrored, the starting position of the microscope slide is then with the objective pointing at bottom right.
Condenser
Generally the condenser is placed in its highest position or just slightly lower. At low magnification objectives (mainly 4x and 10x objectives), the opening of the condenser (or iris) diaphragm should be wide open. For high-dry (40x) and oil-immersion objectives (100x), the diaphragm should be closed slowly while looking at a sharply focused section until the level of illumination is just slightly reduced, in order to attain optimal contrast and resolution.[1]
Artifacts
In microscopy, an artifact is an apparent structural detail that is caused by the processing of the specimen and is thus not a legitimate feature of the specimen. Major artifacts to account for include:
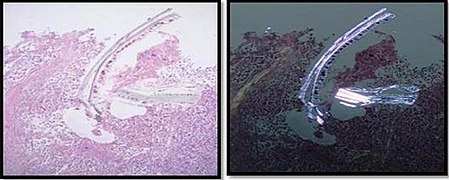
Cellulose contamination, here seen on H&E stain and polarized light, respectively.

Cardiac muscle (bottom) with contamination from thyroid tissue (center).
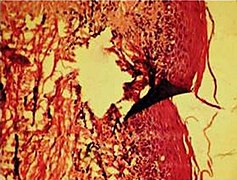
Crush artifact from compression by forceps on the tissue sample.

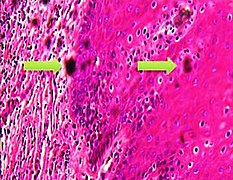
Folding artifacts (white arrows) and a crush artifact (black arrow, with cytoplasmic hypereosinophilia and nuclear pleomorphism) from a needle.

More tearing artifacts, showing that they may be more circular than fusiform.
'Formalin pigment artifacts

Air bubble entrapment artifacts

Staining artifacts by residual wax, resulting in pale areas where cellular structures are not discernible.

A separation artifact in top image makes the tumor look incompletely excised, but the next microtomy level (bottom image) shows a surgical margin of connective tissue.









.jpg)
Notes
- ↑ For a full list of contributors, see article history. Creators of images are attributed at the image description pages, seen by clicking on the images. See Patholines:Authorship for details.
Main page
References
- ↑ Patrice F Spitalnik. Histology Laboratory Manual, Vagelos College of Physicians & Surgeons Columbia University. Retrieved on 2021-09-20.
- ↑ 2.0 2.1 2.2 Taqi, SyedAhmed; Sami, SyedAbdus; Sami, LateefBegum; Zaki, SyedAhmed (2018). "A review of artifacts in histopathology ". Journal of Oral and Maxillofacial Pathology 22 (2): 279. doi:. ISSN 0973-029X.
Image sources