Difference between revisions of "Liver"
m (→Microscopic evaluation in autopsy: ref) |
m (→Acute liver failure: H&E stain) |
||
| Line 48: | Line 48: | ||
Acute liver failure has multiple etiologies, and hence various presentations. Regardless of etiology, the initial hepatic insult that leads to acute liver failure is “hepatitis” in the broadest sense, with extensive hepatocyte injury and necrosis. The initiating process may damage the liver by zonal necrosis (with a centrilobular or acinar zones 3 necrosis being typical of acetaminophen hepatotoxicity), or it may damage the liver by a diffuse hepatitis with necrosis and inflammation as exemplified by acute viral hepatitis A, B, or E infections or other drug hepatotoxicities.<ref name="Lefkowitch2016">{{cite journal|last1=Lefkowitch|first1=Jay H.|title=The Pathology of Acute Liver Failure|journal=Advances In Anatomic Pathology|volume=23|issue=3|year=2016|pages=144–158|issn=1072-4109|doi=10.1097/PAP.0000000000000112}}</ref> | Acute liver failure has multiple etiologies, and hence various presentations. Regardless of etiology, the initial hepatic insult that leads to acute liver failure is “hepatitis” in the broadest sense, with extensive hepatocyte injury and necrosis. The initiating process may damage the liver by zonal necrosis (with a centrilobular or acinar zones 3 necrosis being typical of acetaminophen hepatotoxicity), or it may damage the liver by a diffuse hepatitis with necrosis and inflammation as exemplified by acute viral hepatitis A, B, or E infections or other drug hepatotoxicities.<ref name="Lefkowitch2016">{{cite journal|last1=Lefkowitch|first1=Jay H.|title=The Pathology of Acute Liver Failure|journal=Advances In Anatomic Pathology|volume=23|issue=3|year=2016|pages=144–158|issn=1072-4109|doi=10.1097/PAP.0000000000000112}}</ref> | ||
<gallery mode=packed heights=200> | <gallery mode=packed heights=200> | ||
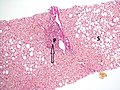
| − | File:Histopathology of acute hepatitis.jpg|Histopathology of acute hepatitis with lobular disarray and associated lymphocytic inflammation, acidophil body formation (arrow) and bilirubinostasis | + | File:Histopathology of acute hepatitis.jpg|Histopathology of acute hepatitis with lobular disarray and associated lymphocytic inflammation, acidophil body formation (arrow) and bilirubinostasis (H&E stain)<ref name="BoydCain2020"/> |
</gallery> | </gallery> | ||
{{Bottom}} | {{Bottom}} | ||
Revision as of 06:03, 20 December 2019
Author:
Mikael Häggström [note 1]
Contents
Tissue sampling
- Autopsy
- Liver biopsy
Fixation
Generally 10% neutral buffered formalin. Non–formalin-fixed tissue may be needed for tests such as microbiological analysis or copper quantification studies.[1]
Gross processing in autopsy
Make consecutive liver slices, such as in the sagittal or coronal plane.
Basic gross examination
- Inspect the color and texture of the surfaces, including external and cut surfaces. Potential pathologies:

Diffuse areas of pallor in cirrhosis, see Cirrhosis

Pale macronodules of cirrhosis, see Cirrhosis

Nutmeg texture of congestive hepatopathy

Liver metastases

.jpg)
.jpg)
.jpg)
- Look for any focal change in the liver volume, mainly any tumor.
- Determine liver weight.
Gross report
- Weight
- Color and texture of cut surfaces
- Any focal change
Microscopic evaluation in autopsy

A minimal screening of autopsy specimens include:
- A severity grading of previously known liver diseases. Quantify any cirrhosis, at least if the patient had alcohol abuse.
- Signs of acute liver failure.
Cirrhosis
Quantification:

No fibrosis, but mild zone 3 steatosis (van Gieson's stain)[1]
Histopathology of steatohepatitis with mild fibrosis in the form of fibrous expansion (van Gieson's stain)[1]

Histopathology of steatohepatitis with moderate fibrosis, with thin fibrous bridges (van Gieson's stain)[1]

Histopathology of steatohepatitis with established cirrhosis, with thick bands of fibrosis (van Gieson's stain)[1]
.jpg)
.jpg)
.jpg)
.jpg)
Acute liver failure
Acute liver failure has multiple etiologies, and hence various presentations. Regardless of etiology, the initial hepatic insult that leads to acute liver failure is “hepatitis” in the broadest sense, with extensive hepatocyte injury and necrosis. The initiating process may damage the liver by zonal necrosis (with a centrilobular or acinar zones 3 necrosis being typical of acetaminophen hepatotoxicity), or it may damage the liver by a diffuse hepatitis with necrosis and inflammation as exemplified by acute viral hepatitis A, B, or E infections or other drug hepatotoxicities.[2]

Histopathology of acute hepatitis with lobular disarray and associated lymphocytic inflammation, acidophil body formation (arrow) and bilirubinostasis (H&E stain)[1]

Notes
- ↑ For a full list of contributors, see article history. Creators of images are attributed at the image description pages, seen by clicking on the images. See Patholines:Authorship for details.
Main page
References
- ↑ 1.0 1.1 1.2 1.3 1.4 1.5 Boyd, Alexander; Cain, Owen; Chauhan, Abhishek; Webb, Gwilym James (2020). "Medical liver biopsy: background, indications, procedure and histopathology
". Frontline Gastroenterology 11 (1): 40–47. doi:. ISSN 2041-4137.
- "This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license"
- ↑ Lefkowitch, Jay H. (2016). "The Pathology of Acute Liver Failure ". Advances In Anatomic Pathology 23 (3): 144–158. doi:. ISSN 1072-4109.
Image sources