Template:Prostate screening method
Contents
Screening method
- Before microscopy, look at each microscopy slide by eye, to plan the microscopy screening so as to not miss peripheral fragments.
- Screen at low power, and switch to high power when encountering glandular structures that can not otherwise be cleared. Look in particular for those surrounding nerves.
- At least if no cancer is seen, also look for inflammation.[notes 1]
Characteristics of adenocarcinoma
- Relatively common and highly specific findings of prostatic adenocarcinoma
- [1]

Multiple nucleoli (Pictured in an acinar adenocarcinoma, the most common subdiagnosis of prostate adenocarcinoma)

Eccentric nucleoli[1] (pictured example has double and eccentric nucleoli).


- Specific but relatively rare signs of adenocarcinoma
- [notes 2]

On biopsies, look in particular near the tips for perineural invasion, as it is most likely seen by the capsule. Glands adjacent to and indenting nerves is not sufficient as a diagnostic criterion by itself. Glands partially surrounding a nerve is an indication of carcinoma.[2]
- Collagenous micronodules for acinar adenocarcinoma[1]
- Angiolymphatic invasion[1]
- Extraprostatic extension,[1] which in biopsies can be diagnosed when tumor cells are located in fatty tissue.
- Less specific findings

Mitoses: also seen in for example high-grade prostatic intraepithelial neoplasia (HGPIN) and prostate inflammation.[1] Picture shows adenocarcinoma with two mitoses in reactive epithelium.

Intraluminal blue mucin[1] (pictured in acinar adenocarcinoma)

Intraluminal atypical eosinophilic secretions.[1]

Intraluminal crystalloids.[3]

Uneven distribution and infiltrative pattern of glands
Glomerulations, for acinar adenocarcinoma, consisting of epithelial proliferations into one or more gland lumina, typically a cribriform tuft with a single attachment to the gland wall.[2]






- Prominent nucleoli[1]
- Nuclear enlargement
Precancerous lesions
,_annotated.jpg)
In case of only less specific findings, consider a Prostatic intraepithelial neoplasia (PIN) or an atypical small acinar proliferation (ASAP).
A PIN is where acini are architecturally benign, but individual cells display atypia. In high-grade PIN (HGPIN), the changes are similar to those of prostate cancer, whereas in low-grade (LGPIN) the changes are milder. Most pathologists do not report the presence of LGPIN.[5]
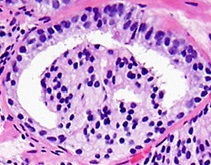
An ASAP is a lesion that is probably carcinoma but either lacks definitive diagnostic features, or is too small to be certain (see image below).[6] It should not be used for benign lesions that are just unusual looking.[6] In uncertain cases, a diagnosis of adenocarcinoma can be excluded by immunohistochemical detection of basal cells (or confirmed by absence thereof),[1] such as using the PIN-4 cocktail of stains (which consists of P504S, p63 and high-molecular-weight keratins (HMWK) such as CK5 and CK14).

Small acinar cell proliferation, with acinar cells with large nuclei, prominent nucleoli (arrows marking two of them) and no certain basal cell lining.

PIN-4 staining of benign prostate gland and adenocarcinoma
.jpg)

Picture above compares a PIN-4 immunohistochemistry of benign gland (left) and adenocarcinoma (right) using PIN-4. The adenocarcinoma lacks the basal epithelial cells (stained dark brown by p63 and HMWK). Also, in PIN-4 stained samples, adenocarcinoma cells generally display red cytoplasms (stained by AMACR, also known as P504S), while benign glands do not.
Notes
Main page
References
- ↑ 1.00 1.01 1.02 1.03 1.04 1.05 1.06 1.07 1.08 1.09 1.10 Cruz, Andrea O.; Santana, Amanda L. S.; Santos, Andréia C.; Athanazio, Daniel A. (2016). "Frequency of the morphological criteria of prostate adenocarcinoma in 387 consecutive prostate needle biopsies: emphasis on the location and number of nucleoli
". Jornal Brasileiro de Patologia e Medicina Laboratorial. doi:. ISSN 1676-2444.
Attribution 4.0 International (CC BY 4.0) license - ↑ 2.0 2.1 2.2 Robert V Rouse MD. Prostatic Adenocarcinoma. Stanford Medical School. Last update 2/2/16
- ↑ Svatek, R S; Karam, J A; Rogers, T E; Shulman, M J; Margulis, V; Benaim, E A (2007). "Intraluminal crystalloids are highly associated with prostatic adenocarcinoma on concurrent biopsy specimens ". Prostate Cancer and Prostatic Diseases 10 (3): 279–282. doi:. ISSN 1365-7852.
- ↑ Image by Mikael Häggström, MD. Reference for features:
- Margaret Sanders, M.B.B.Ch., Murali Varma, M.B.B.S.. High grade prostatic intraepithelial neoplasia (HGPIN). Pathology Outlines. Last author update: 23 February 2021 - ↑ Stanley A Brosman, MD. Precancerous Lesions of the Prostate. Medscape. Updated: Feb 26, 2020
- ↑ 6.0 6.1 . Prostatic Adenocarcinoma - Atypical Small Acinar Proliferation (ASAP). Stanford Medical School. Retrieved on 2020-09-14.
Image sources