Template:Oral and neck
Oral
Jaw cysts
Author:
Mikael Häggström [note 1]
Cystic changes in the jaw bones or around teeth:
Microscopic examination
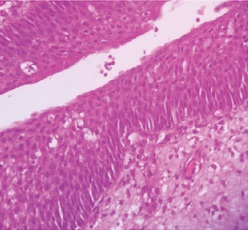
Attempt to characterize the lining of the cyst. Look for important signs:
Signs
![Cholesterol clefts: Indicates of a periapical (radicular) cyst[1] or an inflamed dentigerous cyst[2].](/File:Histopathology_of_cholesterol_clefts_of_a_periapical_cyst_of_the_jaw.jpg)
Any keratinization of the lining.
Any signs of malignancy. Further information: Evaluation of suspected malignancies
Diagnoses

All the following are odontogenic cyst, and in case of inability to specify further, may be simply diagnosed as such:
| Cyst type | Lining epithelium | Other characteristics | Image |
|---|---|---|---|
| Periapical (radicular) cyst | Stratified squamous epithelium of variable thickness, except when originating in a maxillary sinus where there is respiratory epithelium (pseudostratified ciliated columnar epithelium).[1] |
They sometimes have the following features:[1]
|
 |
| Non-inflamed dentigerous cyst | Typically:[2]
They occasionally have:
|

| |
| Inflamed dentigerous cyst | Hyperplastic non-keratinized epithelium[2] | Typically:[2]
Sometimes:[2]
They occasionally have:[2]
|
|
| Residual cyst | Stratified squamous epithelium:[5]
In early cysts, the epithelial lining tend to be proliferative and arcading, with an intense inflammation.
|
Cyst lumen may demonstrate fluid and cellular debris.[5] |
All types above can occasionally have scattered mucous or ciliated cells, as well as Rushton bodies, which are amorphic, eosinophilic, linear to crescent-shaped bodies in the cyst epithelium.[4][1][2][5]
Report
- Type of lining
- Other visible features
- At least the most probable type of cyst.
- Even absence of signs of malignancy
Example:
- Benign odontogenic cyst of periapical type. |
See also: General notes on reporting
Notes
- ↑ For a full list of contributors, see article history. Creators of images are attributed at the image description pages, seen by clicking on the images. See Patholines:Authorship for details.
Main page
References
- ↑ 1.0 1.1 1.2 1.3 1.4 Annie S. Morrison, Kelly Magliocca. Mandible & maxilla - Odontogenic cysts - Periapical (radicular) cyst. Pathology Outlines. Topic Completed: 1 March 2014. Revised: 13 December 2019
- ↑ 2.0 2.1 2.2 2.3 2.4 2.5 2.6 2.7 2.8 Kelly Magliocca, Annie S. Morrison. Mandible & maxilla - Odontogenic cysts - Dentigerous. Pathology Outlines. Topic Completed: 1 October 2013. Revised: 2 December 2019
- ↑ Leandro Bezerra Borges; Francisco Vagnaldo Fechine; Mário Rogério Lima Mota; Fabrício Bitu Sousa; Ana Paula Negreiros Nunes Alves (2012). "Odontogenic lesions of the jaw: a clinical-pathological study of 461 cases. ". Revista Gaúcha de Odontologia 60 (1). Archived from the original. .
- ↑ 4.0 4.1 Tsesis, I; Rosen, E; Dubinsky, L; Buchner, A; Vered, M (2016). "Metaplastic changes in the epithelium of radicular cysts: A series of 711 cases
". Journal of Clinical and Experimental Dentistry: 0–0. doi:. ISSN 19895488.
- "Fig 2- available via license: Creative Commons Attribution 2.5 Generic" - ↑ 5.0 5.1 5.2 Annie S. Morrison, Kelly Magliocca. Mandible & maxilla - Odontogenic cysts - Residual cyst. Pathology Outlines. Topic Completed: 1 April 2014. Revised: 13 December 2019
Image sources
Verrucous oral lesions
Author:
Mikael Häggström [note 1]

Verrucous oral lesions have hypergranulosis and/or hyperkeratosis as the most conspicuous finding.
Microscopic evaluation
Look for signs of koilocyte-like changes, which may indicate verrucous squamous cell carcinoma, and which typically only has low atypia:[1]


Verrucous squamous cell carcinoma (images are from penis).
If uncertain, perform immunohistochemistry for Ki67 and p53.
Notes
- ↑ For a full list of contributors, see article history. Creators of images are attributed at the image description pages, seen by clicking on the images. See Patholines:Authorship for details.
Main page
References
- ↑ Initially copied from: Paolino, Giovanni; Donati, Michele; Didona, Dario; Mercuri, Santo; Cantisani, Carmen (2017). "Histology of Non-Melanoma Skin Cancers: An Update
". Biomedicines 5 (4): 71. doi:. ISSN 2227-9059.
"This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/)."
Image sources
Tonsil
Author:
Mikael Häggström [note 1]
Comprehensiveness
On this resource, the following formatting is used for comprehensiveness:
- Minimal depth
- (Moderate depth)
- ((Comprehensive))
Gross processing

First look at the requisition form ((and in the medical records)) for the following suspicions:
- Suspected infection: Confirm that a sample has been taken for microbiology. If not, take a sample from within the specimen when you gross it.
- Possible lymphoma: Make a touch prep and take sample(s) for flow cytometry. If you have bilateral tonsils, and they look grossly similar, you may combine a small sample of each tonsil into one container for flow cytometry.
- Suspected tumor: Ink the external surfaces before sectioning. Otherwise inking is not needed. Further information: Tumor
Inspect the tonsils for any significant gross focal changes. A representative section of the grossly most abnormal part from each tonsil is generally enough.
- Example gross report
| ((A. Labeled - ___. The specimen is received in formalin and consists of)) one rubbery, ovoid, pink-tan tonsil(s) measuring ____. The mucosal surfaces are unremarkable. On sectioning, the tissue is tan-white and homogenous, with no gross lesions. (Representative sections are submitted for microscopic examination in __ cassettes.) |
Notes
- ↑ For a full list of contributors, see article history. Creators of images are attributed at the image description pages, seen by clicking on the images. See Patholines:Authorship for details.
Main page
References
Image sources
Nasal cavity
Author:
Mikael Häggström [note 1]
Comprehensiveness
On this resource, the following formatting is used for comprehensiveness:
- Minimal depth
- (Moderate depth)
- ((Comprehensive))
Nasal or sinonasal polyps
Look for signs of malignancy. Further information: Evaluation of suspected malignancies

Main differential diagnoses:
-
 Inverted papilloma, wherein the surface epithelial cells grow downward into the underlying supportive tissue.
Inverted papilloma, wherein the surface epithelial cells grow downward into the underlying supportive tissue. -
 Squamous papilloma, with acanthosis and hyperkerratosis.
Squamous papilloma, with acanthosis and hyperkerratosis.


In case of significant inflammation:
- Take at least one high magnification look to confirm that it is mixed and that lymphocytes are not atypical (otherwise, consult hematopathology, particularly whether it could be a lymphoma, notably extranodal NK/T cell lymphoma, nasal type.
- (Classify as acute (with neutrophils) versus chronic (lymphocytes, eosinophils and/or plasma cells). Also look at any bone fragments for osteomyelitis.) Further information: Osteomyelitis
-
 Benign chronic mixed inflammation of an inflammatory sinonasal polyp.
Benign chronic mixed inflammation of an inflammatory sinonasal polyp. -
 Acute inflammation characterized by neutrophils.
Acute inflammation characterized by neutrophils. -
![Extranodal NK/T cell lymphoma, nasal type.[2] These lymphoma cells are typically monotonous, with folded nuclei, indistinct nucleoli and moderate amount of cytoplasm.[3]](https://upload.wikimedia.org/wikipedia/commons/c/c4/Histopathology_of_extranodal_NK-T_cell_lymphoma%2C_nasal_type.png)


![Extranodal NK/T cell lymphoma, nasal type.[2] These lymphoma cells are typically monotonous, with folded nuclei, indistinct nucleoli and moderate amount of cytoplasm.[3]](/File:Histopathology_of_extranodal_NK-T_cell_lymphoma,_nasal_type.png)
Reporting
Example:
 Benign respiratory mucosa with chronic inflammation. Bone without significant histopathologic changes. |
Notes
- ↑ For a full list of contributors, see article history. Creators of images are attributed at the image description pages, seen by clicking on the images. See Patholines:Authorship for details.
Main page
References
- ↑ Michaels, Leslie (2012-12-06) (in en). Ear, Nose and Throat Histopathology . Springer Science & Business Media. p. 168. ISBN 9781447133322.
- ↑ Takahara M, Kumai T, Kishibe K, Nagato T, Harabuchi Y (2021). "Extranodal NK/T-Cell Lymphoma, Nasal Type: Genetic, Biologic, and Clinical Aspects with a Central Focus on Epstein-Barr Virus Relation.
". Microorganisms 9 (7). doi:. PMID 34202088. PMC: 8304202. Archived from the original. .
- "This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/)." - ↑ Mario L. Marques-Piubelli, M.D., Carlos A. Torres-Cabala, M.D., Roberto N. Miranda, M.D.. Extranodal NK / T cell lymphoma, nasal type. Pathology Outlines. Last author update: 5 January 2021. Last staff update: 14 October 2021
Image sources
Salivary glands
Author:
Mikael Häggström, M.D. [note 1]
The major salivary glands are the parotid, submandibular, and sublingual glands.
Evaluation
Look for the most common tumors:
-
![Relative incidence of parotid tumors.[1]](https://upload.wikimedia.org/wikipedia/commons/thumb/b/b1/Relative_incidence_of_parotid_tumors.png/960px-Relative_incidence_of_parotid_tumors.png) Relative incidence of parotid tumors.[1]
Relative incidence of parotid tumors.[1] -
![Relative incidence of submandibular tumors.[1]](https://upload.wikimedia.org/wikipedia/commons/thumb/a/a7/Relative_incidence_of_submandibular_tumors.png/960px-Relative_incidence_of_submandibular_tumors.png) Relative incidence of submandibular tumors.[1]
Relative incidence of submandibular tumors.[1] -
![Pleomorphic adenoma (also called benign mixed tumor), H&E stain.[2]](https://upload.wikimedia.org/wikipedia/commons/thumb/8/8a/Histopathology_of_pleomorphic_adenoma.png/500px-Histopathology_of_pleomorphic_adenoma.png) Pleomorphic adenoma (also called benign mixed tumor), H&E stain.[2]
Pleomorphic adenoma (also called benign mixed tumor), H&E stain.[2]
![Relative incidence of parotid tumors.[1]](/File:Relative_incidence_of_parotid_tumors.png)
![Relative incidence of submandibular tumors.[1]](/File:Relative_incidence_of_submandibular_tumors.png)
![Pleomorphic adenoma (also called benign mixed tumor), H&E stain.[2]](/File:Histopathology_of_pleomorphic_adenoma.png)
Cytology
-
![Pleomorphic adenoma (Pap stain). It can usually be diagnosed by its typical fibrillary stroma (mesenchyme). Stromal cell nuclei are small. Myoepithelial cells are usually the predominant cell type, and can have various shapes but are usually more elongated than epithelial cells. Epithelial cells may have prominent nucleoli.[3]](https://upload.wikimedia.org/wikipedia/commons/thumb/8/83/Cytopathology_of_pleomorphic_adenoma.png/500px-Cytopathology_of_pleomorphic_adenoma.png) Pleomorphic adenoma (Pap stain). It can usually be diagnosed by its typical fibrillary stroma (mesenchyme). Stromal cell nuclei are small. Myoepithelial cells are usually the predominant cell type, and can have various shapes but are usually more elongated than epithelial cells. Epithelial cells may have prominent nucleoli.[3]
Pleomorphic adenoma (Pap stain). It can usually be diagnosed by its typical fibrillary stroma (mesenchyme). Stromal cell nuclei are small. Myoepithelial cells are usually the predominant cell type, and can have various shapes but are usually more elongated than epithelial cells. Epithelial cells may have prominent nucleoli.[3] -
![Warthin's tumor, with typical cellular features (and relatively uncommon binucleated cells).[4] Pap stain. For a diagnosis, you should see sheets of oncocytes and a mixed population of lymphocytes.[5]](https://upload.wikimedia.org/wikipedia/commons/thumb/e/e7/Cytopathology_of_Warthin%27s_tumor.jpg/960px-Cytopathology_of_Warthin%27s_tumor.jpg)
![Pleomorphic adenoma (Pap stain). It can usually be diagnosed by its typical fibrillary stroma (mesenchyme). Stromal cell nuclei are small. Myoepithelial cells are usually the predominant cell type, and can have various shapes but are usually more elongated than epithelial cells. Epithelial cells may have prominent nucleoli.[3]](/File:Cytopathology_of_pleomorphic_adenoma.png)
![Warthin's tumor, with typical cellular features (and relatively uncommon binucleated cells).[4] Pap stain. For a diagnosis, you should see sheets of oncocytes and a mixed population of lymphocytes.[5]](/File:Cytopathology_of_Warthin%27s_tumor.jpg)
Reporting=
Example report:
| Right parotid mass, biopsy: – Pleomorphic adenoma. |
Notes
- ↑ For a full list of contributors, see article history. Creators of images are attributed at the image description pages, seen by clicking on the images. See Patholines:Authorship for details.
Main page
References
- ↑ 1.0 1.1 Steve C Lee, MD, PhD. Salivary Gland Neoplasms. Medscape. Updated: Jan 13, 2021}}
Diagrams by Mikael Häggström, MD - ↑ Image by Mikael Häggström, MD. Reference for description: Bin Xu, M.D., Ph.D.. Pleomorphic adenoma. Pathology Outlines. Last author update: 30 July 2021. Last staff update: 6 February 2023
- ↑ Image by Mikael Häggström, MD. Reference for description: Bin Xu, M.D., Ph.D.. Pleomorphic adenoma. Last author update: 30 July 2021. Last staff update: 5 August 2021
- ↑ Image by Mikael Häggström, MD. References for entries:
- Köybaşioğlu FF, Önal B, Han Ü, Adabağ A, Şahpaz A (2020). "Cytomorphological findings in diagnosis of Warthin tumor ". Turk J Med Sci 50 (1): 148-154. doi:. PMID 31769640. PMC: 7080357. Archived from the original. .
Binucleation:
- Dr.S. Malliga (2006-10-18). A correlative cytological and histopathological study on lesions of salivary gland.
- Chan MKM, McGuire LJ: Cytodiagnosis of Lesions Presenting as Salivary Gland Swellings: A Report of Seven Cases. Diagn Cytopathol 8: 439-443, 1992b. - ↑ Adriana Handra-Luca, M.D., Ph.D., Jen-Fan Hang, M.D.. Warthin tumor. Pathology Outlines. Last author update: 1 September 2012. Last staff update: 28 June 2022
Image sources
Thyroid
Fixation
Generally 10% neutral buffered formalin. Fix all thyroids at least overnight to avoid artifactual nuclear atypia.[1]
See also: General notes on fixation
Removal during autopsy

Sharply dissect the thyroid from the cartilage, starting at the posterior end of each lobe & working forward. Do not cut the isthmus. Try to find parathyroids.
Gross processing of thyroidectomy
- Weigh.[2] Up to 30 g versus over 30 g grams is an accepted cutoff between normal and increased weight of the thyroid gland.[3]
- Measure each lobe and isthmus in 3 dimensions, respectively.[2]
- Ink outer surface,[2] at least if malignancy is suspected.[4]
-
 Hemithyroidecomy (lobe + isthmus) or lobectomy, including completion thyroidectomies: Use separate colors over the cut surface and the outer “capsular” or "peripheral" surface.
Hemithyroidecomy (lobe + isthmus) or lobectomy, including completion thyroidectomies: Use separate colors over the cut surface and the outer “capsular” or "peripheral" surface. -
 None of the outer “capsular” surface should be inked like the cut surface.
None of the outer “capsular” surface should be inked like the cut surface. -
 Intact total thyroidectomy: Separate colors for each lobe and the isthmus.
Intact total thyroidectomy: Separate colors for each lobe and the isthmus. -
 If no appreciable isthmus, Separate colors for each lobe.
If no appreciable isthmus, Separate colors for each lobe.




((In addition, use different ink colors on the anterior versus posterior “capsular” or "peripheral" surface.))
Serially section the specimen at 3-4mm intervals,[5] such as follows:[2]
-
 Hemithyroidecomy (lobe + isthmus) or lobectomy: Include isthmic orange margins in your transverse sections.
Hemithyroidecomy (lobe + isthmus) or lobectomy: Include isthmic orange margins in your transverse sections. -
 Intact total thyroidectomy: Transverse lobe sections and sagittal isthmus sections
Intact total thyroidectomy: Transverse lobe sections and sagittal isthmus sections -
 Short/inconspicious isthmus: The isthmus can be included in the transverse sections.
Short/inconspicious isthmus: The isthmus can be included in the transverse sections.



See also: General notes on gross processing
-
 Thyroiditis, defined by a significant inflammatory infiltrate, usually lymphocytic.
Thyroiditis, defined by a significant inflammatory infiltrate, usually lymphocytic. -
![Thyroid hyperplasia: Variable sized dilated follicles with flattened to hyperplastic epithelium. May form nodules, but without any significant capsule. Architecture resembles normal thyroid, but may be somewhat hypercellular.[6]](https://upload.wikimedia.org/wikipedia/commons/thumb/5/50/Histopathology_of_nodular_hyperplasia_of_the_thyroid.png/960px-Histopathology_of_nodular_hyperplasia_of_the_thyroid.png) Thyroid hyperplasia: Variable sized dilated follicles with flattened to hyperplastic epithelium. May form nodules, but without any significant capsule. Architecture resembles normal thyroid, but may be somewhat hypercellular.[6]
Thyroid hyperplasia: Variable sized dilated follicles with flattened to hyperplastic epithelium. May form nodules, but without any significant capsule. Architecture resembles normal thyroid, but may be somewhat hypercellular.[6] -
![Thyroid follicular adenoma, being architecturally and cytologically different from surrounding gland, and being completely enveloped by thin fibrous capsule (if not being encapsulated, mainly consider thyroid carcinoma if atypical cells, otherwise nodular hyperplasia with dominant nodule, the latter especially if there are hyperplastic changes elsewhere in gland).[7] Hyperfunctioning follicular adenoma typically shows follicles with papillary infoldings and bubbly, pale colloid with peripheral scalloping (a). Non-hyperfunctioning adenomas with papillary hyperplasia usually show a more predominantly papillary pattern without vacuolated cytoplasm and scalloping colloid (b).[8]](https://upload.wikimedia.org/wikipedia/commons/thumb/6/63/Histopathology_of_hyperfunctioning_and_non-hyperfunctioning_thyroid_follicular_adenoma.jpg/960px-Histopathology_of_hyperfunctioning_and_non-hyperfunctioning_thyroid_follicular_adenoma.jpg) Thyroid follicular adenoma, being architecturally and cytologically different from surrounding gland, and being completely enveloped by thin fibrous capsule (if not being encapsulated, mainly consider thyroid carcinoma if atypical cells, otherwise nodular hyperplasia with dominant nodule, the latter especially if there are hyperplastic changes elsewhere in gland).[7] Hyperfunctioning follicular adenoma typically shows follicles with papillary infoldings and bubbly, pale colloid with peripheral scalloping (a). Non-hyperfunctioning adenomas with papillary hyperplasia usually show a more predominantly papillary pattern without vacuolated cytoplasm and scalloping colloid (b).[8]
Thyroid follicular adenoma, being architecturally and cytologically different from surrounding gland, and being completely enveloped by thin fibrous capsule (if not being encapsulated, mainly consider thyroid carcinoma if atypical cells, otherwise nodular hyperplasia with dominant nodule, the latter especially if there are hyperplastic changes elsewhere in gland).[7] Hyperfunctioning follicular adenoma typically shows follicles with papillary infoldings and bubbly, pale colloid with peripheral scalloping (a). Non-hyperfunctioning adenomas with papillary hyperplasia usually show a more predominantly papillary pattern without vacuolated cytoplasm and scalloping colloid (b).[8] -
![NIFTP (noninvasive follicular thyroid neoplasm with papillary-like nuclear features): [9]](https://upload.wikimedia.org/wikipedia/commons/thumb/7/7b/Histopathology_of_NIFTP.png/960px-Histopathology_of_NIFTP.png) NIFTP (noninvasive follicular thyroid neoplasm with papillary-like nuclear features): [9]
NIFTP (noninvasive follicular thyroid neoplasm with papillary-like nuclear features): [9] -
![Hürthle cell adenoma, typically consisting of cells with large size, distinct cell borders, deeply eosinophilic and granular cytoplasm, large nucleus with prominent nucleolus, and complete loss of cell polarity.[10]](https://upload.wikimedia.org/wikipedia/commons/thumb/a/ae/Histopathology_of_a_H%C3%BCrthle_cell_adenoma.jpg/500px-Histopathology_of_a_H%C3%BCrthle_cell_adenoma.jpg) Hürthle cell adenoma, typically consisting of cells with large size, distinct cell borders, deeply eosinophilic and granular cytoplasm, large nucleus with prominent nucleolus, and complete loss of cell polarity.[10]
Hürthle cell adenoma, typically consisting of cells with large size, distinct cell borders, deeply eosinophilic and granular cytoplasm, large nucleus with prominent nucleolus, and complete loss of cell polarity.[10] -
 Relative incidences of malignant thyroid tumors.
Relative incidences of malignant thyroid tumors.

![Thyroid hyperplasia: Variable sized dilated follicles with flattened to hyperplastic epithelium. May form nodules, but without any significant capsule. Architecture resembles normal thyroid, but may be somewhat hypercellular.[6]](/File:Histopathology_of_nodular_hyperplasia_of_the_thyroid.png)
![Thyroid follicular adenoma, being architecturally and cytologically different from surrounding gland, and being completely enveloped by thin fibrous capsule (if not being encapsulated, mainly consider thyroid carcinoma if atypical cells, otherwise nodular hyperplasia with dominant nodule, the latter especially if there are hyperplastic changes elsewhere in gland).[7] Hyperfunctioning follicular adenoma typically shows follicles with papillary infoldings and bubbly, pale colloid with peripheral scalloping (a). Non-hyperfunctioning adenomas with papillary hyperplasia usually show a more predominantly papillary pattern without vacuolated cytoplasm and scalloping colloid (b).[8]](/File:Histopathology_of_hyperfunctioning_and_non-hyperfunctioning_thyroid_follicular_adenoma.jpg)
![NIFTP (noninvasive follicular thyroid neoplasm with papillary-like nuclear features): [9]](/File:Histopathology_of_NIFTP.png)
![Hürthle cell adenoma, typically consisting of cells with large size, distinct cell borders, deeply eosinophilic and granular cytoplasm, large nucleus with prominent nucleolus, and complete loss of cell polarity.[10]](/File:Histopathology_of_a_H%C3%BCrthle_cell_adenoma.jpg)

Papillary thyroid carcinoma
A papillary thyroid carcinoma is characterized by:
-
 Pseudonuclear inclusions (representing cytoplasmic invaginations)
Pseudonuclear inclusions (representing cytoplasmic invaginations) -
 Nuclear grooves
Nuclear grooves


Also, it typically has nuclei with:[11]
- Enlargement, elongation, overlapping
- Chromatin with clearing, margination, glassy / ground glass texture
- Nuclear membrane with irregular contour
Other thyroid tumors
-
![Follicular thyroid carcinoma, resembling follicular cells, and typically do not display the nuclear features of papillary thyroid carcinoma mentioned above. Distinction from adenoma requires invasion of adjacent thyroid parenchyma, capsule (complete penetration) and/or blood vessels (in or beyond the capsule).[12]](https://upload.wikimedia.org/wikipedia/commons/thumb/d/da/Histopathology_of_follicular_thyroid_carcinoma.png/500px-Histopathology_of_follicular_thyroid_carcinoma.png) Follicular thyroid carcinoma, resembling follicular cells, and typically do not display the nuclear features of papillary thyroid carcinoma mentioned above. Distinction from adenoma requires invasion of adjacent thyroid parenchyma, capsule (complete penetration) and/or blood vessels (in or beyond the capsule).[12]
Follicular thyroid carcinoma, resembling follicular cells, and typically do not display the nuclear features of papillary thyroid carcinoma mentioned above. Distinction from adenoma requires invasion of adjacent thyroid parenchyma, capsule (complete penetration) and/or blood vessels (in or beyond the capsule).[12]
![Follicular thyroid carcinoma, resembling follicular cells, and typically do not display the nuclear features of papillary thyroid carcinoma mentioned above. Distinction from adenoma requires invasion of adjacent thyroid parenchyma, capsule (complete penetration) and/or blood vessels (in or beyond the capsule).[12]](/File:Histopathology_of_follicular_thyroid_carcinoma.png)
Reporting
For cancers, generally include a synoptic report, such as per College of American Pathologists (CAP) protocols at cap.org/protocols-and-guidelines.
See also: General notes on reporting
Thyroiditis
Papillary thyroid carcinoma
Evaluation

A papillary thyroid carcinoma is characterized by:
-
Pseudonuclear inclusions (representing cytoplasmic invaginations)
-
Nuclear grooves
Also, it typically has nuclei with:[13]
- Enlargement, elongation, overlapping
- Chromatin with clearing, margination, glassy / ground glass texture
- Nuclear membrane with irregular contour
Staging
Staging as per AJCC, 8th edition:[14]
| T Category | T Criteria |
|---|---|
| TX | Primary tumor cannot be assessed |
| T0 | No evidence of primary tumor |
| T1 | Tumor ≤2 cm in greatest dimension limited to the thyroid |
| T1a | Tumor ≤1 cm in greatest dimension limited to the thyroid |
| T1b | Tumor >1 cm but ≤2 cm in greatest dimension limited to the thyroid |
| T2 | Tumor >2 cm but ≤4 cm in greatest dimension limited to the thyroid |
| T3 | Tumor >4 cm limited to the thyroid, or gross extrathyroidal extension invading only strap muscles |
| T3a | Tumor >4 cm limited to the thyroid |
| T3b | Gross extrathyroidal extension invading only strap muscles (sternohyoid, sternothyroid, thyrohyoid, or omohyoid muscles) from a tumor of any size |
| T4 | Includes gross extrathyroidal extension beyond the strap muscles |
| T4a | Gross extrathyroidal extension invading subcutaneous soft tissues, larynx, trachea, esophagus, or recurrent laryngeal nerve from a tumor of any size |
| T4b | Gross extrathyroidal extension invading prevertebral fascia or encasing the carotid artery or mediastinal vessels from a tumor of any size |
| N Category | N Criteria |
|---|---|
| NX | Regional lymph nodes cannot be assessed |
| N0 | No evidence of locoregional lymph node metastasis |
| N0a | One or more cytologically or histologically confirmed benign lymph nodes |
| N0b | No radiologic or clinical evidence of locoregional lymph node metastasis |
| N1 | Metastasis to regional nodes |
| N1a | Metastasis to level VI or VII (pretracheal, paratracheal, or prelaryngeal/Delphian, or upper mediastinal) lymph nodes. This can be unilateral or bilateral disease. |
| N1b | Metastasis to unilateral, bilateral, or contralateral lateral neck lymph nodes (levels I, II, III, IV, or V) or retropharyngeal lymph nodes |
| M Category | M Criteria |
|---|---|
| M0 | No distant metastasis |
| M1 | Distant metastasis |
Thyroid cytology
Author:
Mikael Häggström [note 1]
Adequacy
A minimum number of 6 clusters with 10 cells each has been arbitrary established to assume adequacy for a definitive diagnosis.[15] The presence of characteristic cells may still confer a definitive diagnosis, but otherwise, the report will simply state inadequate number of cells.
Risk stratification
Look at least for the following imaged features, and classify findings as per the Bethesda system:
| Category | Description[16] | Example report |
|---|---|---|
| I | Non diagnostic/unsatisfactory | |
| II | Benign (colloid and follicular cells) | Thyroid aspiration, right upper pole:
|
| III | Atypia of undetermined significance (AUS) or follicular lesion of undetermined significance (FLUS) (follicular or lymphoid cells with atypical features) | Thyroid aspiration, right mid pole:
|
| IV | Follicular nodule/suspicious follicular nodule (cell crowding, micro follicles, dispersed isolated cells, scant colloid) | |
| V | Suspicious for malignancy | |
| VI | Malignant |
-
![Relative incidences of histopathologic diagnoses of solitary thyroid nodules that have undergone fine needle aspiration.[17]](https://upload.wikimedia.org/wikipedia/commons/thumb/6/66/Relative_incidences_of_histopathologic_diagnoses_of_solitary_thyroid_nodules.png/500px-Relative_incidences_of_histopathologic_diagnoses_of_solitary_thyroid_nodules.png) Relative incidences of histopathologic diagnoses of solitary thyroid nodules that have undergone fine needle aspiration.[17]
Relative incidences of histopathologic diagnoses of solitary thyroid nodules that have undergone fine needle aspiration.[17] -
 Cytology of benign follicular epithelial cells (Bethesda category II), Pap stain, showing cells with significant nuclear pleomorphism but otherwise insignificant features.
Cytology of benign follicular epithelial cells (Bethesda category II), Pap stain, showing cells with significant nuclear pleomorphism but otherwise insignificant features. -
![Look for microfollicles, which are flat groups of follicular cells, each having less than 15 follicular cells arranged in a circle that is at least two thirds complete.[18][image 1] They indicate a follicular neoplasm.](https://upload.wikimedia.org/wikipedia/commons/d/dc/Cytology_of_microfollicles.jpg)
-
![Thyroid spherules, on the other hand, are benign features. A spherule may mimic a microfollicle, but has a more smooth, round, ball-like contour, and even spacing of the follicular cell nuclei.[19]](https://upload.wikimedia.org/wikipedia/commons/thumb/1/13/Cytology_of_thyroid_spherule.jpg/500px-Cytology_of_thyroid_spherule.jpg) Thyroid spherules, on the other hand, are benign features. A spherule may mimic a microfollicle, but has a more smooth, round, ball-like contour, and even spacing of the follicular cell nuclei.[19]
Thyroid spherules, on the other hand, are benign features. A spherule may mimic a microfollicle, but has a more smooth, round, ball-like contour, and even spacing of the follicular cell nuclei.[19] -
Relative incidences of malignant thyroid tumors.
-
![Cytopathology suspicious for Hürthle cell neoplasm (Bethesda category IV), Pap stain. However, it cannot distinguish Hürthle cell adenoma from Hürthle cell carcinoma, which requires histopathologic sections to see transcapsular or vascular invasion. Hürthle cell hyperplasia (as seen in Hashimoto's thyroiditis) may show moderate variation in nuclear sizes and prominent nucleoli, but further findings favoring Hürthle cell neoplasm include a large number of Hürthle cells, and discohesiveness.[20]](https://upload.wikimedia.org/wikipedia/commons/thumb/6/65/Cytopathology_suspicious_for_H%C3%BCrthle_cell_neoplasm%2C_annotated.png/960px-Cytopathology_suspicious_for_H%C3%BCrthle_cell_neoplasm%2C_annotated.png) Cytopathology suspicious for Hürthle cell neoplasm (Bethesda category IV), Pap stain. However, it cannot distinguish Hürthle cell adenoma from Hürthle cell carcinoma, which requires histopathologic sections to see transcapsular or vascular invasion. Hürthle cell hyperplasia (as seen in Hashimoto's thyroiditis) may show moderate variation in nuclear sizes and prominent nucleoli, but further findings favoring Hürthle cell neoplasm include a large number of Hürthle cells, and discohesiveness.[20]
Cytopathology suspicious for Hürthle cell neoplasm (Bethesda category IV), Pap stain. However, it cannot distinguish Hürthle cell adenoma from Hürthle cell carcinoma, which requires histopathologic sections to see transcapsular or vascular invasion. Hürthle cell hyperplasia (as seen in Hashimoto's thyroiditis) may show moderate variation in nuclear sizes and prominent nucleoli, but further findings favoring Hürthle cell neoplasm include a large number of Hürthle cells, and discohesiveness.[20]
![Relative incidences of histopathologic diagnoses of solitary thyroid nodules that have undergone fine needle aspiration.[17]](/File:Relative_incidences_of_histopathologic_diagnoses_of_solitary_thyroid_nodules.png)

![Look for microfollicles, which are flat groups of follicular cells, each having less than 15 follicular cells arranged in a circle that is at least two thirds complete.[18][image 1] They indicate a follicular neoplasm.](/File:Cytology_of_microfollicles.jpg)
![Thyroid spherules, on the other hand, are benign features. A spherule may mimic a microfollicle, but has a more smooth, round, ball-like contour, and even spacing of the follicular cell nuclei.[19]](/File:Cytology_of_thyroid_spherule.jpg)
![Cytopathology suspicious for Hürthle cell neoplasm (Bethesda category IV), Pap stain. However, it cannot distinguish Hürthle cell adenoma from Hürthle cell carcinoma, which requires histopathologic sections to see transcapsular or vascular invasion. Hürthle cell hyperplasia (as seen in Hashimoto's thyroiditis) may show moderate variation in nuclear sizes and prominent nucleoli, but further findings favoring Hürthle cell neoplasm include a large number of Hürthle cells, and discohesiveness.[20]](/File:Cytopathology_suspicious_for_H%C3%BCrthle_cell_neoplasm,_annotated.png)
Notes
- ↑ For a full list of contributors, see article history. Creators of images are attributed at the image description pages, seen by clicking on the images. See Patholines:Authorship for details.
Main page
References
- ↑ . Gross Pathology Manual By The University of Chicago Department of Pathology. Updated 2-14-19 NAC.
- ↑ 2.0 2.1 2.2 2.3 . Gross Pathology Manual By The University of Chicago Department of Pathology. Updated 2-14-19 NAC.
- ↑ Shamim, A; Monira, K; Manowara, B; Sabiha, M; Alim, A; Nurunnabi, ASM (1970). "Weight of the Human Thyroid Gland A Postmortem Study
". Bangladesh Journal of Medical Science 9 (1): 44–48. doi:. ISSN 2076-0299.
- In turn citing: Langer P. Discussion about the limit between normal thyroid and goiter: mini review. Endocrine regulations. 1999 March; 33(1): 39-45. - ↑ Monica Dahlgren, Janne Malina, Anna Måsbäck, Otto Ljungberg. Stora utskärningen. KVAST (Swedish Society of Pathology). Retrieved on 2019-09-26.
- ↑ . THYROID. Royal College of pathologists of Australia. Retrieved on 2019-12-17.
- ↑ Swati Satturwar, M.D., F. Zahra Aly, M.D., Ph.D.. Thyroid & parathyroid - Hyperplasia / goiter - Multinodular goiter. PathologyOutlines. Last author update: 11 June 2021. Last staff update: 18 November 2021
- ↑ Sheren Younes, M.D.. Thyroid & parathyroid Benign thyroid neoplasms. Follicular adenoma.. Pathology Outlines. Last author update: 1 November 2014. Last staff update: 8 March 2022
- ↑ Cameselle-Teijeiro JM, Eloy C, Sobrinho-Simões M (2020). "Pitfalls in Challenging Thyroid Tumors: Emphasis on Differential Diagnosis and Ancillary Biomarkers.
". Endocr Pathol 31 (3): 197-217. doi:. PMID 32632840. PMC: 7395918. Archived from the original. .
"This article is licensed under a Creative Commons Attribution 4.0 International License" - ↑ Image by Mikael Häggström, MD. Reference for findings: Rachel Jug, M.B.B.Ch., B.A.O., David Poller, M.D., Xiaoyin "Sara" Jiang, M.D.. NIFTP. Pathology Outlines. Last author update: 10 May 2018
- ↑ Shuanzeng (Sam) Wei, M.D., Ph.D.. Thyroid & parathyroid - Other thyroid carcinoma - Main- Oncocytic (Hürthle cell) tumors. Pathology Outlines. Last author update: 1 October 2017. Last staff update: 21 July 2021
- ↑ Bin Xu, M.D., Ph.D.. Thyroid & parathyroid - Papillary thyroid carcinoma - Papillary thyroid carcinoma overview. Pathology Outlines. Topic Completed: 8 January 2020. Minor changes: 28 May 2021
- ↑ Shuanzeng (Sam) Wei, M.D., Ph.D.. Thyroid & parathyroid - Other thyroid carcinoma - Follicular. Pathology Outlines. Last author update: 1 August 2017. Last staff update: 24 May 2022
- ↑ Bin Xu, M.D., Ph.D.. Thyroid & parathyroid - Papillary thyroid carcinoma - Papillary thyroid carcinoma overview. Pathology Outlines. Topic Completed: 8 January 2020. Minor changes: 28 May 2021
- ↑ Amin, Mahul (2017). AJCC cancer staging manual
(8 ed.). Switzerland: Springer. ISBN 978-3-319-40617-6. OCLC 961218414.
- For access, see the Secrets chapter of Patholines.
- Copyright note: The AJCC, 8th Ed. is published by a company in Switzerland, and the tables presented therein are Public Domain because they consist of tabular information without literary or artistic innovation, and therefore do not fulfil the inclusion criterion of the Swiss Copyright Act (CopA) which applies to "literary and artistic intellectual creations with individual character" (see Federal Act on Copyright and Related Rights (Copyright Act, CopA) of 9 October 1992 (Status as of 1 January 2022)). - ↑ Michael, Claire W.; Pang, Yijun; Pu, Robert T.; Hasteh, Farnaz; Griffith, Kent A. (2007). "Cellular adequacy for thyroid aspirates prepared by ThinPrep: How many cells are needed? ". Diagnostic Cytopathology 35 (12): 792–797. doi:. ISSN 87551039.
- ↑ "The bethesda system for reporting thyroid cytopathology: interpretation and guidelines in surgical treatment ". Indian Journal of Otolaryngology and Head and Neck Surgery 64 (4): 305–311. December 2012. doi:. PMID 24294568.
- ↑ Diagram by Mikael Häggström, MD. Source data: Arul P, Masilamani S (2015). "A correlative study of solitary thyroid nodules using the bethesda system for reporting thyroid cytopathology. ". J Cancer Res Ther 11 (3): 617-22. doi:. PMID 26458591. Archived from the original. .
- ↑ Ayana Suzuki, C.T., Andrey Bychkov, M.D., Ph.D.. Thyroid & parathyroid - Follicular neoplasm. Last author update: 21 April 2022. Last staff update: 12 May 2022
- ↑ Costigan DC, Shaar M, Frates MC, Alexander EK, Barletta JA, Cibas ES (2020). "Defining thyroid spherules: A benign cytomorphologic feature that mimics microfollicles. ". Cancer Cytopathol 128 (3): 171-176. doi:. PMID 31856389. Archived from the original. .
- ↑ Image by Mikael Häggström, MD. References for findings:
- Ayana Suzuki, C.T., Andrey Bychkov, M.D., Ph.D.. Hürthle cell neoplasm. Pathology Outlines. Last author update: 7 May 2020. Last staff update: 12 May 2022
- Shawky M, Sakr M (2016). "Hurthle Cell Lesion: Controversies, Challenges, and Debates. ". Indian J Surg 78 (1): 41-8. doi:. PMID 27186039. PMC: 4848220. Archived from the original. .
Image sources
- ↑ . 4. 2021. Archived from Sharma Avishesh Singh , Ajay Sahu the original. .
- "This is an Open Access article that uses a funding model which does not charge readers or their institutions for access and distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0)"
Parathyroid glands
Author:
Mikael Häggström [note 1]
Presentations
Intraoperative consultation
Necessary components are:
- Weight of the parathyroid gland or fragment thereof. Generally, there should not be any subjective description of "enlarged" or similar.[note 2]
- Presence of parathyroid tissue upon frozen section. In particular, exclude sampling from the thyroid. It is not necessary to specify any particular parathyroid pathology on intraoperative consultation (which in case of hyperparathyroidism relies on imaging and intraoperative parathyroid hormone levels rather than the histopathology)[1].
Autopsy
Optionally for a comprehensive autopsy, or where there is suspicion of parathyroid pathology, an effort is made to find the parathyroid glands, and inspect them for general or focal hyper-/neoplasia.
Microscopic evaluation
The main conditions to look for and distinguish are:
- Parathyroid hyperplasia: Typically involves all 4 glands with diffuse enlargement.[2]
- Parathyroid adenoma: Typically nodular growth with compressed rim of normal tissue.[2]
Either is indicated by a decreased amount of intra-gland adipose tissue, and increased weight. A weight of 35-160 mg is above average but not in itself "enlarged" in the absence of other findings.[note 2]
-
 Histology of the parathyroid glands
Histology of the parathyroid glands -
![Parathyroid chief cell hyperplasia: An increase in the parenchymal cell mass,as a result of the proliferation of chief cells, oncocytes, and transitional oncocytes in multiple parathyroid glands.[3]](https://upload.wikimedia.org/wikipedia/commons/c/c9/Histopathology_of_parathyroid_chief_cell_hyperplasia.jpg) Parathyroid chief cell hyperplasia: An increase in the parenchymal cell mass,as a result of the proliferation of chief cells, oncocytes, and transitional oncocytes in multiple parathyroid glands.[3]
Parathyroid chief cell hyperplasia: An increase in the parenchymal cell mass,as a result of the proliferation of chief cells, oncocytes, and transitional oncocytes in multiple parathyroid glands.[3] -
 Parathyroid adenoma, with chief cells and eosinophilic follicles
Parathyroid adenoma, with chief cells and eosinophilic follicles -
 Parathyroid adenoma, fine needle aspiration
Parathyroid adenoma, fine needle aspiration

![Parathyroid chief cell hyperplasia: An increase in the parenchymal cell mass,as a result of the proliferation of chief cells, oncocytes, and transitional oncocytes in multiple parathyroid glands.[3]](/File:Histopathology_of_parathyroid_chief_cell_hyperplasia.jpg)

.jpg)
Microscopy report
Example for an intraoperative consultation:
| A. Left inferior parathyroid, excision: 24 mg of parathyroid tissue. C. Right superior parathyroid, excision: |
Whenever possible, make a single report for multiple fragments from the same location. Example of final report, including additional fragments from the same locations:
| A,B. Left inferior parathyroid gland, excision: Hypercellular parathyroid gland (121 mg aggregate weight), consistent with parathyroid hyperplasia. C,D. Right superior parathyroid gland, excision: E. Left superior parathyroid gland, excision: F. Right inferior parathyroid gland, excision: |
Normal example in autopsy:
| Sections show <<1, 2, 3, 4>> parathyroid glands with no focal changes or signs of hyperplasia. |
Cite error: <ref> tags exist for a group named "note", but no corresponding <references group="note"/> tag was found
- ↑ Naik AH, Wani MA, Wani KA, Laway BA, Malik AA, Shah ZA (2018). "Intraoperative Parathyroid Hormone Monitoring in Guiding Adequate Parathyroidectomy. ". Indian J Endocrinol Metab 22 (3): 410-416. doi:. PMID 30090736. PMC: 6063190. Archived from the original. .
- ↑ 2.0 2.1 Diana Murro Lin. Thyroid & parathyroid - Parathyroid nonmalignant - Parathyroid adenoma. Pathology Outlines. Topic Completed: 27 October 2020. Minor changes: 2 June 2021.
- ↑ Piciucchi, Sara; Barone, Domenico; Gavelli, Giampaolo; Dubini, Alessandra; Oboldi, Devil; Matteuci, Federica (2012). "Primary Hyperparathyroidism: Imaging to Pathology
". Journal of Clinical Imaging Science 2: 59. doi:. ISSN 2156-7514.
- This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.